(UroToday.com) The 2024 South Central AUA annual meeting included a session on bladder cancer, featuring a presentation by Dr. Cheryl Lee discussing the case for bladder sparing therapy for high risk non muscle invasive bladder cancer (NMIBC). Radical cystectomy offers excellent local control for NMIBC patients, with local recurrence rates of <5%. It also remains the most effective monotherapy for muscle invasive bladder cancer, with a 50%-70% overall survival rate for clinical T2 disease, and 85%-90% overall survival rate for those downstaged after cystectomy to pathologic NMIBC. However, there remains concern for the morbidity of radical cystectomy, which may be as high as a >50%-60% complication rate, as well as a compromised quality of life.
The new 2024 AUA updated guidelines for NMIBC recognize intravesical therapy for front line disease in high risk NMIBC, as well as in patients with BCG unresponsive disease, with the following updated recommendations:
Statement 15: In a high-risk patient with newly diagnosed CIS, high-grade T1, or high-risk Ta urothelial carcinoma, a clinician should administer a six-week induction course of BCG. (Strong Recommendation; Evidence Strength: Grade B).
Statement 26. In a patient with persistent or recurrent high-grade NMIBC within 12 months of completion of adequate BCG therapy (two induction courses or one induction course plus one maintenance cycle) who is unwilling or unfit for cystectomy, a clinician may recommend clinical trial enrollment, an alternative intravesical therapy (i.e. nadofaragene firadenovec) or alternative intravesical chemotherapies (gemcitabine/docetaxel). A clinician may also offer systemic immunotherapy with pembrolizumab to a patient with CIS within 12 months of completion of adequate BCG therapy. (Conditional Recommendation; Evidence Strength: Grade C).
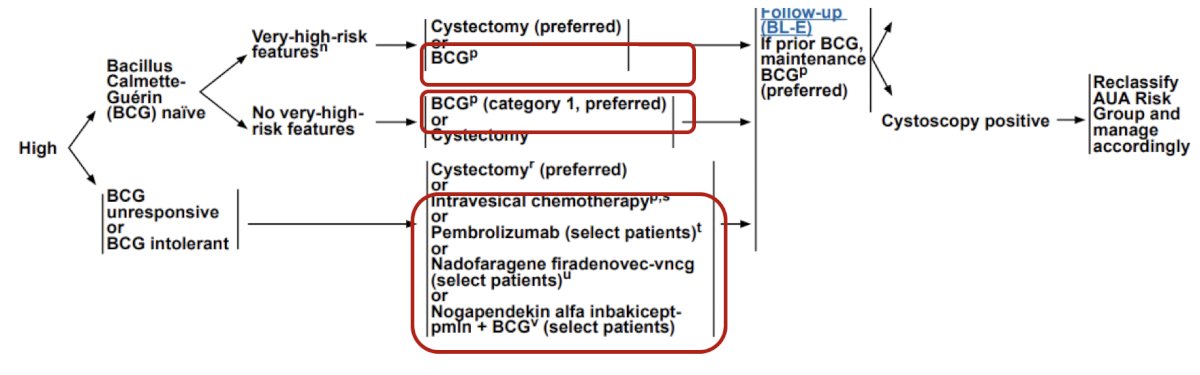
Moreover, the NCCN guidelines support the utilization of bladder sparing options for BCG naïve patients with and without very high risk features, as well as for BCG unresponsive or intolerant patients:
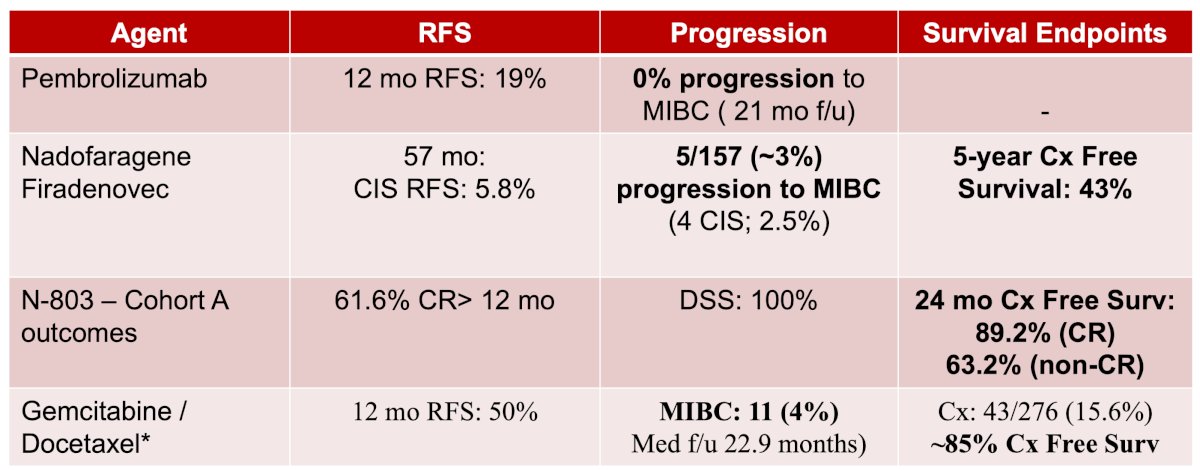
Across all NMIBC risk groups, Dr. Lee notes that the risk of recurrence is high, with 12-24 month recurrence rates of 30% for low risk, ~40% for intermediate risk, and 40-60% for high risk disease. Particularly high risk features include any BCG failure in a high grade patient, any variant histology, any lymphovascular invasion, and any high grade prostatic urethral involvement. The real concern for these patients is the risk of disease progression. Among patients with CIS of the bladder, the progression risk is 5-15% at 5 years, however in the trials highlighted below, progression rates and cystectomy free survival rates are quite good:
For high grade T1 disease, risk stratification is critical. Understaging occurs in ~10-30% of patients, with a 5-year recurrence rate of 42%, 5-year progression rate of 21%, and 5-year cancer specific survival rate of 87%. Additional important stratification points include: (i) genomic risk, (ii) depth of invasion (T1b/c > T1), (iii) associated CIS, LVI, variant histology, (iv) multifocal/high volume disease, and (v) persistent T1 disease after re-TURBT. Patients with high volume T1, variant histology, and/or LVI have a high risk of progression at 1 year (similar to high risk NMIBC at 5 years), and a 5 year progression rate of 15-40%.
Dr. Lee concluded her presentation by discussing the case for bladder sparing therapy for high risk NMIBC with the following take-home points:
- Bladder sparing strategies are justified in high risk NMIBC
- Greater patient selection is required for very high risk NMIBC
- Novel agents can salvage BCG unresponsive CIS patients with low short-term progression rates
- There is an expanding role of bladder sparing, but radical cystectomy remains the ultimate salvage treatment
Presented by: Cheryl Lee, MD, The Ohio State University, Columbus, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 South Central American Urological Association (AUA) Annual Meeting, Colorado Springs, CO, Wed, Oct 30 – Sat, Nov 2, 2024.