(UroToday.com) The 2024 South Central AUA annual meeting included a session on kidney cancer, featuring a presentation by Dr. Frances Alba discussing nephron sparing surgery for localized renal masses. Dr. Alba started by emphasizing that a partial nephrectomy for small renal masses is associated with excellent oncologic outcomes and excellent renal function outcomes.
Additionally, it is the only nephron sparing approach that offers relative oncologic certainty by yielding complete pathological information about the excised tumor. Indeed, we know that partial nephrectomy is great, but Dr. Alba notes that it is not so straight forward with complex or aggressive tumors.
With regards to oncologic efficacy, partial nephrectomy is associated with more favorable recurrence free survival when compared to single session tumor ablation. For cT1a tumors, partial nephrectomy and repeat tumor ablation have similar outcomes, whereas for cT1b tumors partial nephrectomy is generally favored. Based on work from Andrews et al.1 cancer specific survival and metastasis free survival is excellent for all nephron sparing modalities. Overall survival is dependent on an individual patient’s comorbidity and concurrent risk factors. Shared decision making for the appropriate nephron sparing approach is important given that from an oncologic perspective, in low stage disease, clinically relevant differences between treatments is unlikely.
Discussing renal function outcomes, Dr. Alba noted that partial nephrectomy is associated with less decline in postoperative GFR and a lower incidence of chronic kidney disease stage 3 when compared to radical nephrectomy, but similar when compared to tumor ablation. Post partial nephrectomy renal function is impacted by kidney quality, remnant quantity, and ischemia type and duration. Urologists tend to overlook proteinuria in the evaluation of chronic kidney disease, with albuminuria having a dramatic influence on all cause and cardiovascular mortality, independent of eGFR:2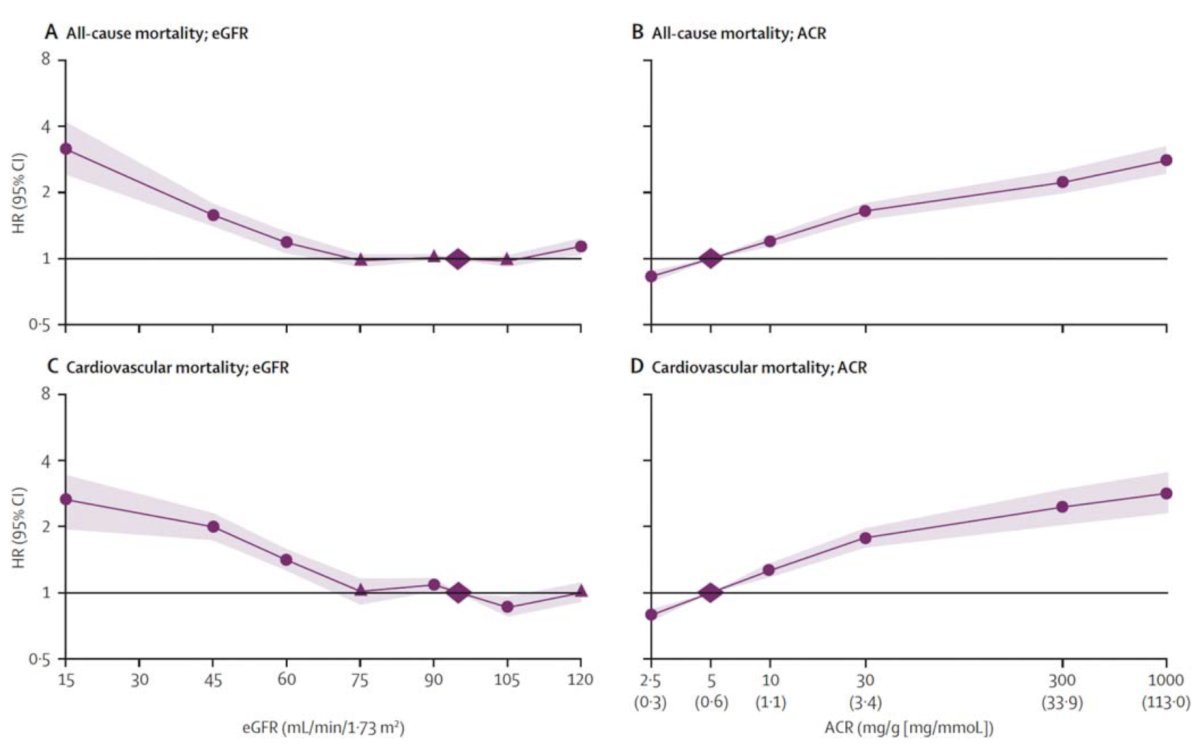
Indeed, proteinuria is an independent prognosticator for overall survival and kidney function, and those with medical and surgical chronic kidney disease fair worse in terms of non oncological survival compared to those with only surgical chronic kidney disease: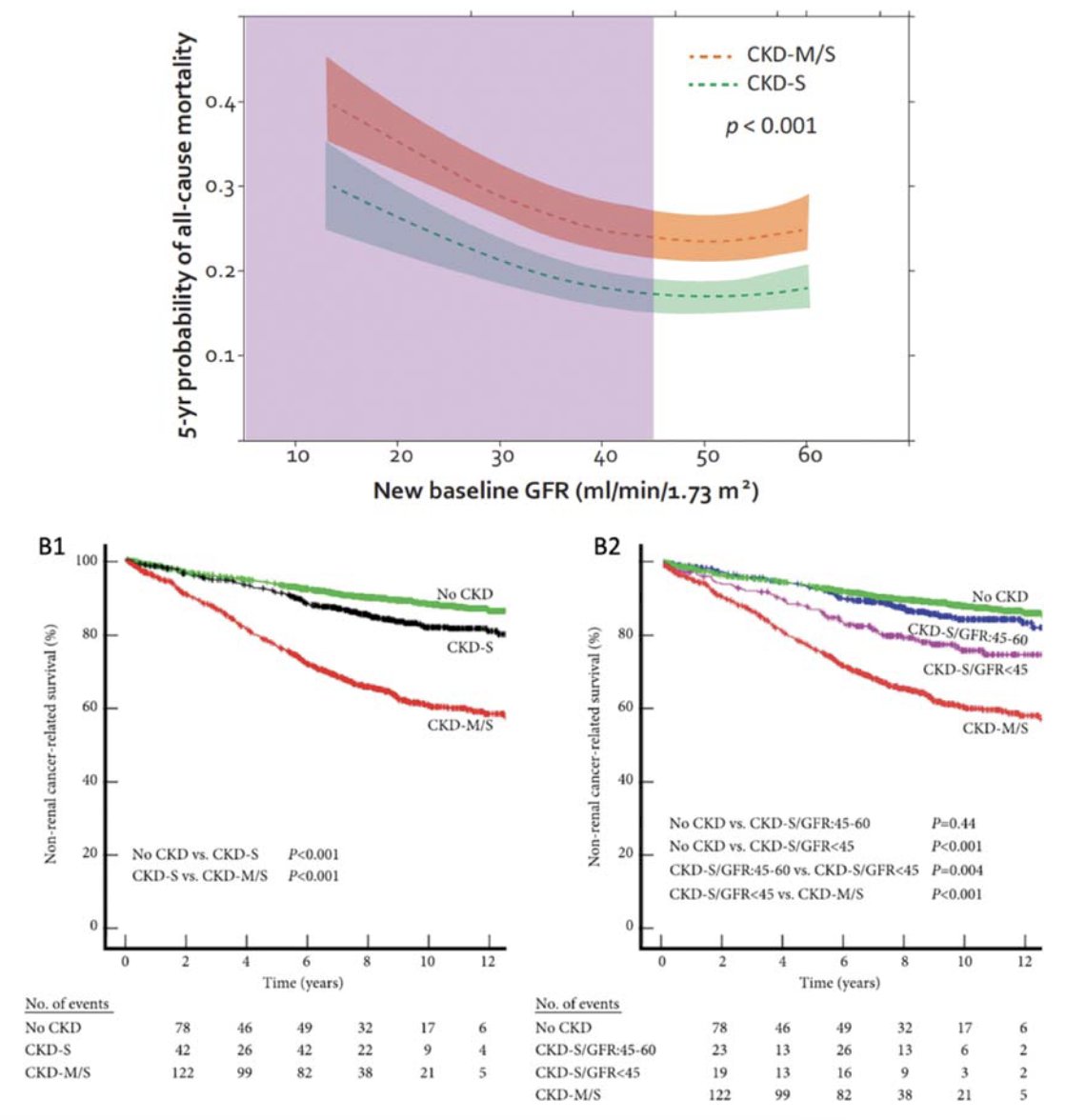
The main procedural related renal complications of partial nephrectomy include urine leak and hemorrhage. Urine leak occurs in 4-5% of cases, and most can be successfully managed conservatively with a stent or a drain. Factors associated with a urine leak including increasing tumor size and proximity to the collecting system. Partial nephrectomy is associated with increased incidence of blood transfusion compared to ablation modalities and radical nephrectomy. Risk factors for hemorrhage include:
- Coagulopathy
- Vascular injury
- Proximity to the collecting system
- Tumor size (<= 4 cm: 6.3% transfusion rate; >4 cm: 14.6% transfusion rate)
In her practice, Dr. Alba notes that we cannot control anatomical or patient related factors, but we can choose the best approach to optimize oncologic control, renal function preservation, and minimizing morbidity.
Dr. Alba concluded her presentation discussing nephron sparing surgery for localized renal masses with the following take-home points highlighting the importance of factors associated with performing a successful partial nephrectomy:
- Anatomical: is it cT1b? Endophytic or exophytic? Close to the collecting system? Lower pole?
- Is it a solitary kidney? (either anatomically or functionally)
- Patient related factors: baseline CKD, medical comorbidities, etc
- Warm ischemia time: ideally 25-30 minutes maximum
- Quantity of the renal parenchyma that is preserved: may affect margin status, decision to enucleate, etc
- Familial RCC: is the patient at risk for bilateral, multifocal tumors, and recurrence?
- Higher likelihood of needing multiple interventions throughout their life
Presented by: Frances Alba, MD, University of New Mexico, Albuquerque, NM
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 South Central American Urological Association (AUA) Annual Meeting, Colorado Springs, CO, Wed, Oct 30 – Sat, Nov 2, 2024.
References:
- Andrews JR, Atwell T, Schmit G, et al. Oncologic outcomes following partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur Urol. 2019 Aug;76(2):244-251.
- Huang WC, Donin NM, Levey AS, et al. Chronic kidney disease and kidney cancer surgery: New perspectives. J Urol. 2020 Mar;203(3):475-485.