(UroToday.com) The Advanced Prostate Cancer Consensus Conference 2021 meeting session discussing the management of newly diagnosed metastatic hormone-sensitive prostate cancer (mHSPC) included a discussion of the nine key panel questions specific to the mHSPC disease space. Dr. Bertrand Tombal and Dr. Nicholas James started with the results of question #12: In the majority of patients with synchronous high-volume (on conventional imaging or unequivocal on next-generation imaging) mHSPC, what is your preferred systemic treatment in addition to ADT?
- AR pathway inhibitor (abiraterone/apalutamide/enzalutamide) as sole additional therapy (49% of respondents)
- Docetaxel as the sole additional therapy (11% of respondents)
- Docetaxel plus an AR pathway inhibitor (abiraterone/apalutamide/enzalutamide) (40% of respondents)
- ADT alone (0% of respondents)
- Abstain (0% of respondents)

Question #13 then asked In the majority of patients with metachronous high-volume (on conventional imaging or unequivocal on next-generation imaging) mHSPC, what is your preferred systemic treatment in addition to ADT?
- AR pathway inhibitor (abiraterone/apalutamide/enzalutamide) as sole additional therapy (71% of respondents)
- Docetaxel as the sole additional therapy (7% of respondents)
- Docetaxel plus an AR pathway inhibitor (abiraterone/apalutamide/enzalutamide) (21% of respondents)
- ADT alone (1% of respondents)
- Abstain (0% of respondents)

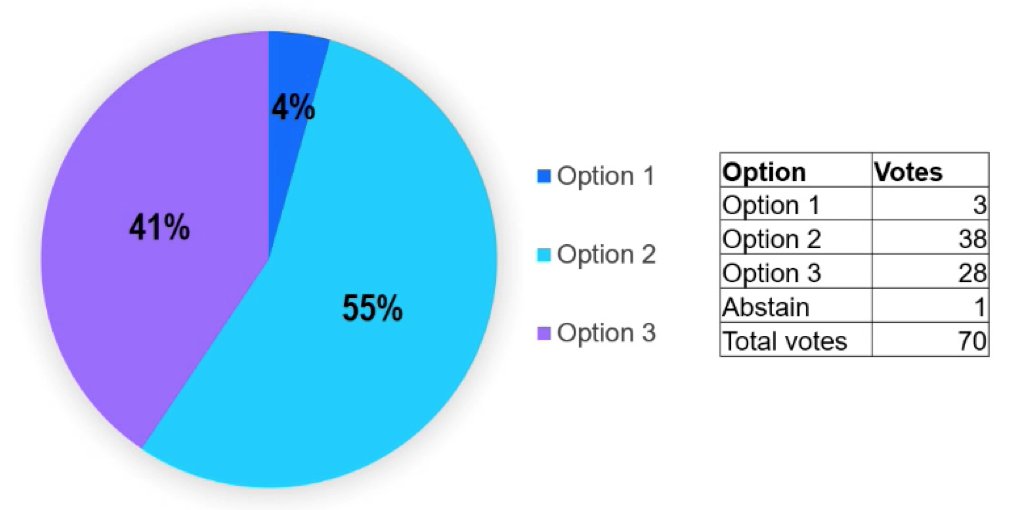
Question #29 asked In which patients with synchronous mHSPC that are chemotherapy fit, do you recommend the triplet therapy ADT plus docetaxel plus abiraterone (in addition to ADT)?
- In the majority of patients independent of disease volume (4% of respondents)
- Only in high-volume patients (55% of respondents)
- I usually do not recommend this combination (41% of respondents)
- Abstain (1 respondent)
Questions #31 asked In which patients with mHSPC that are chemotherapy fit, do you recommend the triplet therapy ADT plus docetaxel plus enzalutamide or apalutamide?
- In the majority of patients independent of disease volume and disease stage (synchronous and metachronous)? (0% of respondents)
- Only in high-volume patients independent of disease stage (21% of respondents)
- Only in synchronous high-volume patients (19% of respondents)
- I usually do not recommend this combination (60% of respondents)
- Abstain (3 respondents)

Question #28 asked What is your recommended treatment strategy, in the majority of patients with mHSPC that have low-volume disease by conventional imaging but high-volume by next-generation imaging?
- Treat as per high-volume (47% of respondents)
- Treat as per low-volume (53% of respondents)
- Abstain (0% of respondents)

Question #15 asked In the majority of patients with symptoms from the primary tumor with synchronous low-volume (conventional imaging) mHSPC, what is your preferred treatment in addition to ADT?
- Additional systemic therapy (8% of respondents)
- Radical local treatment of the primary tumor (+/- metastases directed therapy) (14% of respondents)
- Radical local treatment of the primary tumor plus additional systemic therapy (+/- metastases directed therapy) (77% of respondents)
- No additional treatment (ADT alone) (1% of respondents)
- Abstain (0% of respondents)

Question #6 asked For local treatment of the primary tumor in mHSPC, what is the cut-off of the number of bone metastases based on conventional imaging for recommending local treatment of the primary tumor?
- 3 or less bone metastases (64% of respondents)
- 5 or less bone metastases (29% of respondents)
- No upper limit of bone metastases (6% of respondents)
- I don’t recommend local treatment of the primary in the metastatic setting (1% of respondents)
- Abstain (1 respondent)

Question #38 asked In patients with mHSPC with a poor response to ADT and docetaxel (PSA of >4 after 6 cycles of docetaxel) do you recommend adding an AR pathway inhibitor at this time point and not wait for the development of CRPC?
- Yes (59% of respondents)
- No (41% of respondents)
- Abstain (2 respondents)

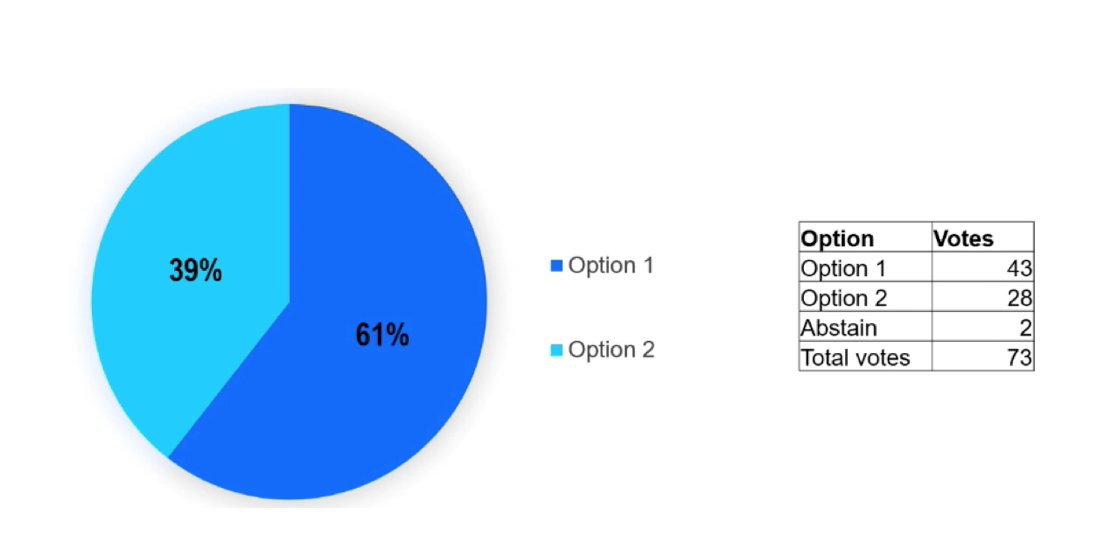
Finally, question #39 asked In patients with mHSPC with durable deep remission to systemic treatment with PSA undetectable (e.g. <= 0.2 ng/mL at 2-3 years), do you discuss with the patient the possibility of stopping all systemic therapy (ADT +/- AR pathway inhibitor)?
- Yes (61% of respondents)
- No (39% of respondents)
- Abstain (2 respondents)
Presented by:
- Nicholas D. James, MBBS, FRCP, FRCR, PhD, Institute of Cancer Research and the Royal Marsden NHS Foundation Trust, London, UK
- Bertrand Tombal, MD, PhD, Urology, Cliniques universitaires Saint-Luc, UC Louvain, Brussels, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 Advanced Prostate Cancer Consensus Conference, Saturday, October 9, 2021.