(UroToday.com) The 2024 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a session on the treatment for biochemical recurrence/PSA persistence, and a presentation by Dr. Daniel Spratt discussing what additional systemic therapy and duration of treatment are required for patients who receive salvage radiation therapy for biochemical recurrence.
Dr. Spratt notes that it is important to personalize ADT post-operatively, with the focus of his talk on salvage radiotherapy and salvage radiotherapy + ADT. In the salvage radiotherapy +/- hormone therapy space there have been four key trials, including RTOG 9601,1 GETUG-16,2 SPPORT/RTOG 0534,3 and RADICALS-HD. The main results of these trials are generally two-fold:
- For early salvage radiotherapy (PSA 0.1-0.5 ng/mL), hormone therapy does not clearly improve overall survival
- For late salvage radiotherapy (PSA >= 0.5 ng/mL), long-term hormone therapy may improve overall survival
The take-home messages from these trials, according to Dr. Spratt, are that not all patients with PSA recurrence after surgery should be treated the same and that many do not need ADT.
Previously, the NRG/RTOG 9601 trial1 showed that two years of high-dose bicalutamide improved overall survival: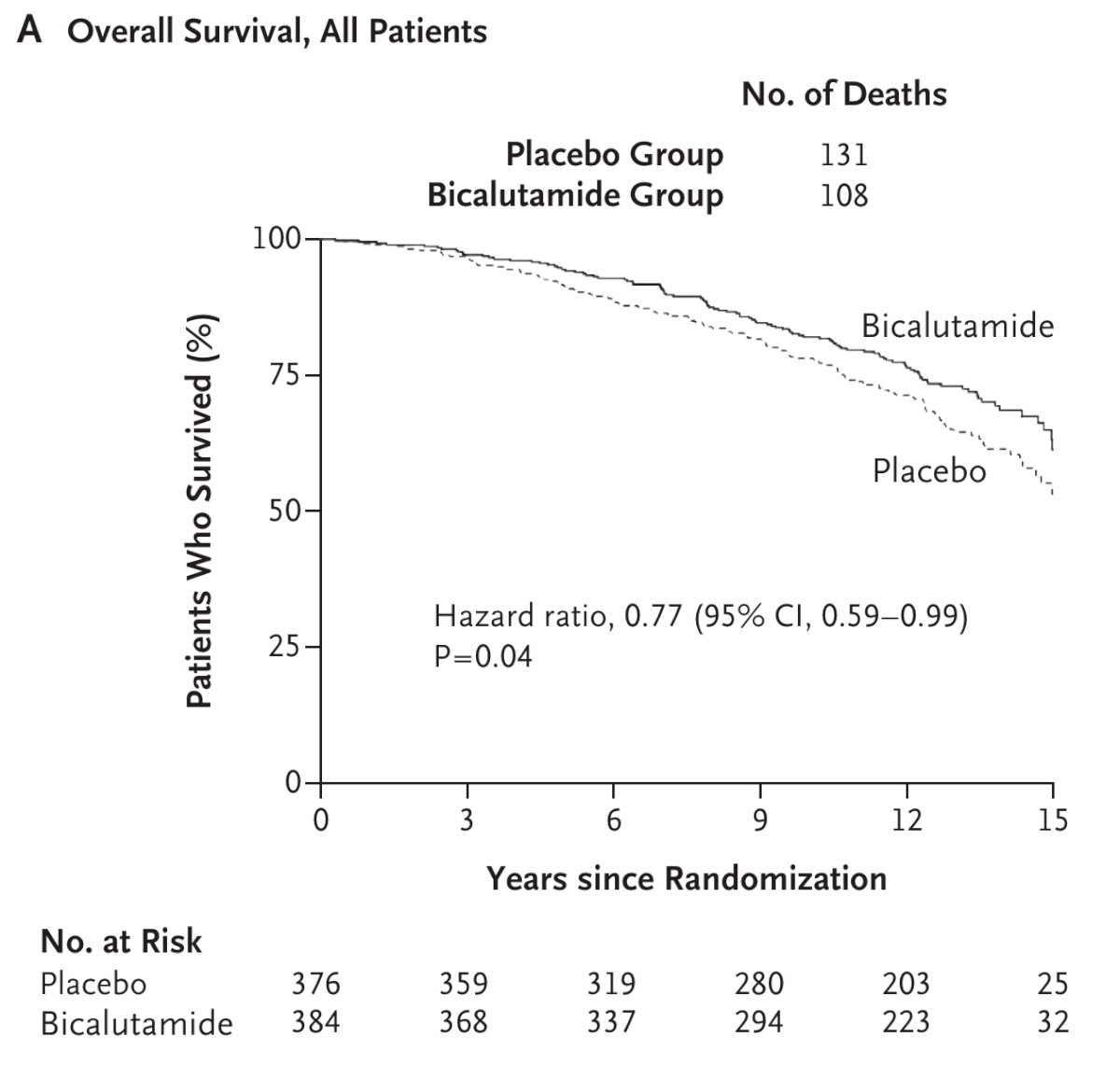
However, in this somewhat historical trial, the median entry PSA was 1.5 ng/mL, which is notably higher than current clinical practice. Thus, it is not surprising that those with a PSA of 1.6-4.0 ng/mL derived a benefit from bicalutamide (p = 0.01), compared to those with a PSA of 0.2-1.5 ng/mL (p = 0.36) who did not (encompassing 85% of patients in the trial):4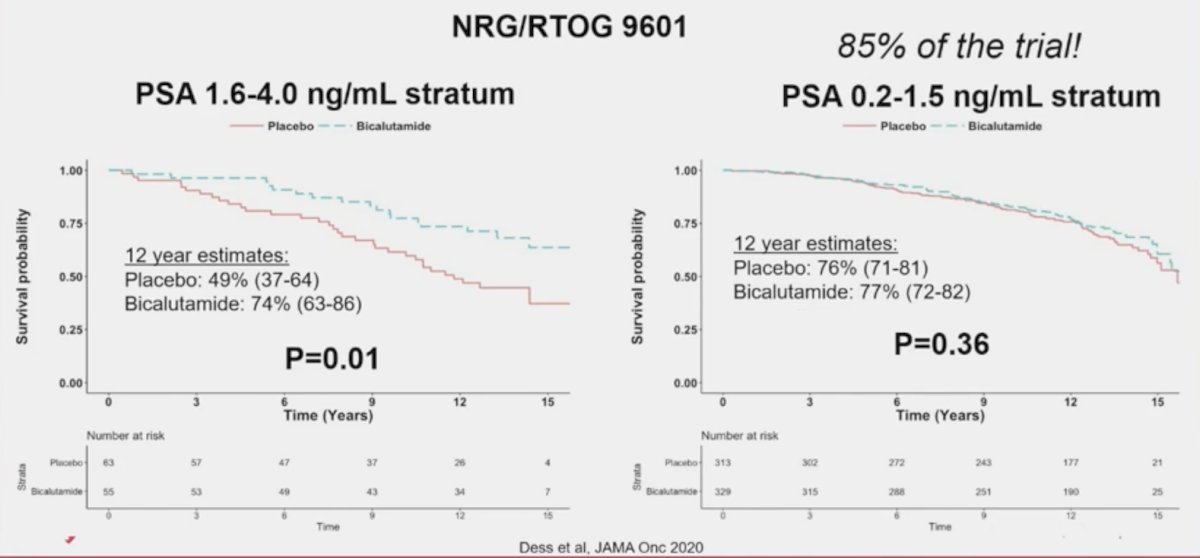
In not only RTOG 9601 but also in GETUG-16 and SPPORT, among patients with PSAs less than ~1.5 ng/mL there is no clear survival benefit from adding ADT: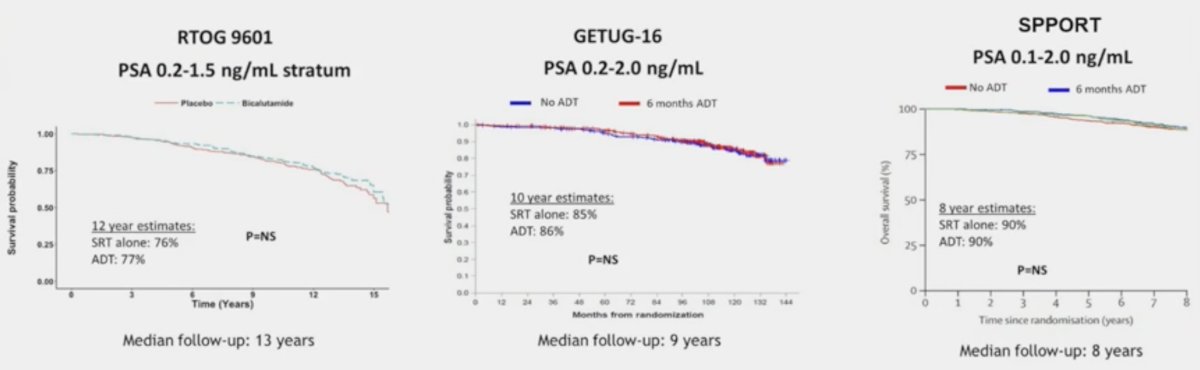
In a meta-analysis of RTOG 9601 (excluding patients with high PSAs), GETUG-16, and RTOG 0534, again, there was a consistent lack of overall survival benefit for the addition of ADT: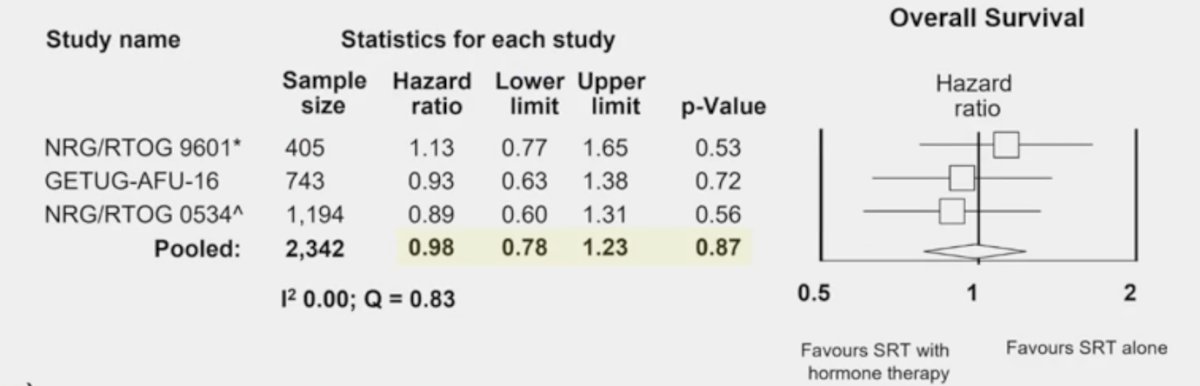
Moreover, in the RADICALS-HD assessment of radiotherapy +/- short term ADT, there was no benefit to metastasis-free survival or overall survival for the addition of ADT: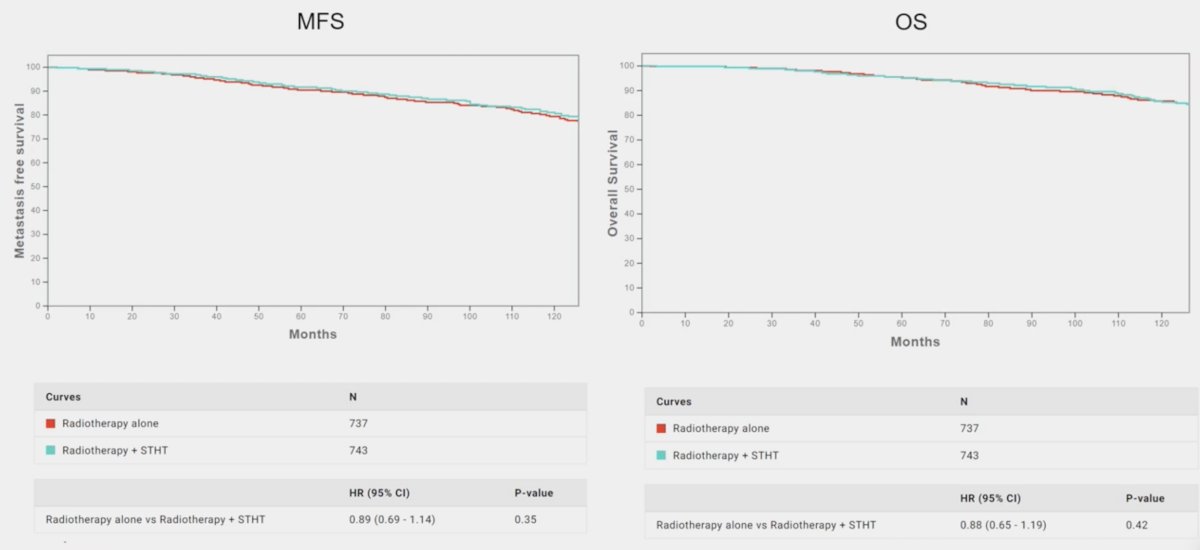
In the RADICALS-HD comparison of short- vs long duration of ADT, based on 313 events, 24 months of ADT improved metastasis-free survival (HR 0.77; CI: 0.61-0.97; 72% vs 78% at 10 years), however, there was no benefit in overall survival. Dr. Spratt notes that perhaps the metastasis-free survival benefit for long-term ADT is somewhat unclear: when compared to radiotherapy alone, the HR for radiotherapy + long-term ADT is 0.94 (95% CI 0.53-1.68).
Generally, for pre-salvage radiotherapy, PSA is consistently the most prognostic variable: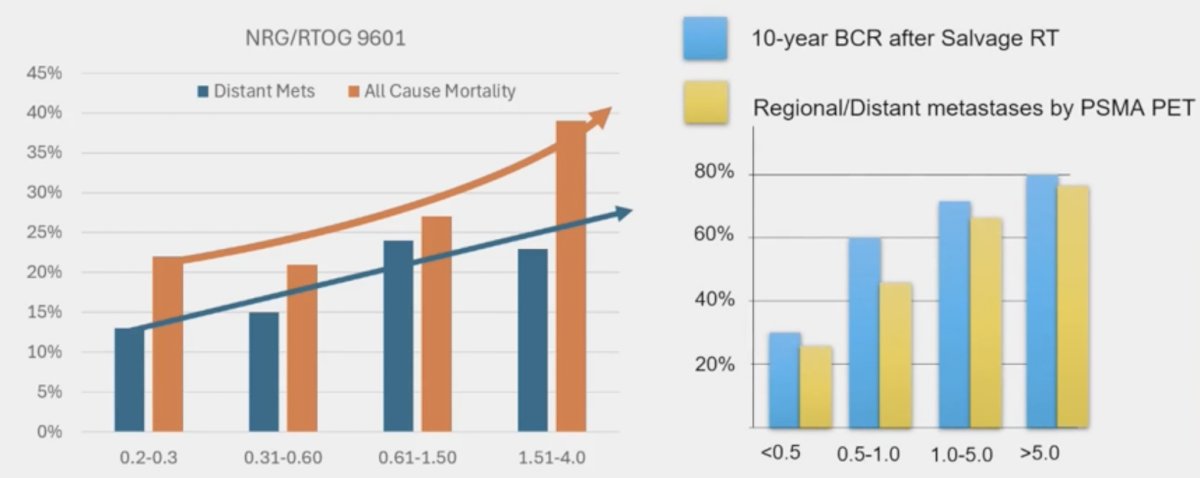
Moreover, the differential benefit by pre-salvage radiotherapy PSA is seen in NRG/RTOG 9601 for overall survival and distant metastasis: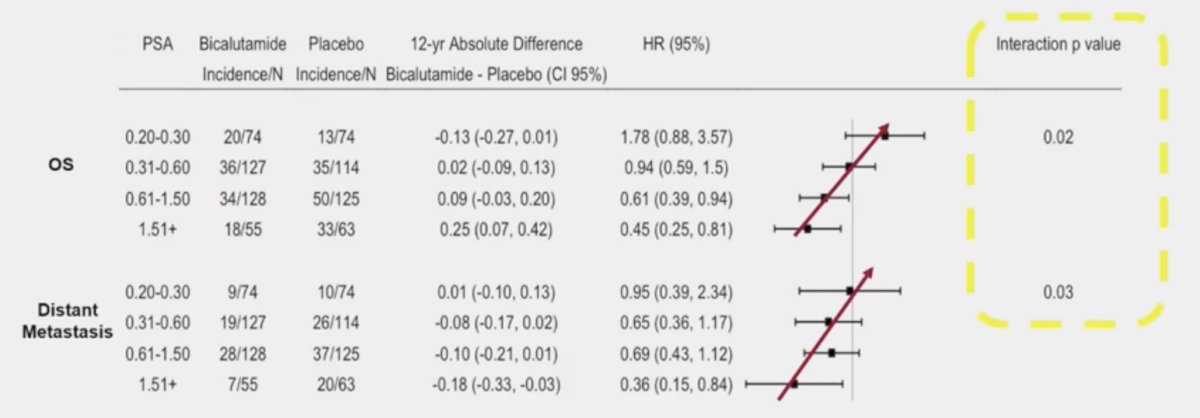
This also appears to be consistent for biochemical progression-free survival in:
GETUG-AFU-16: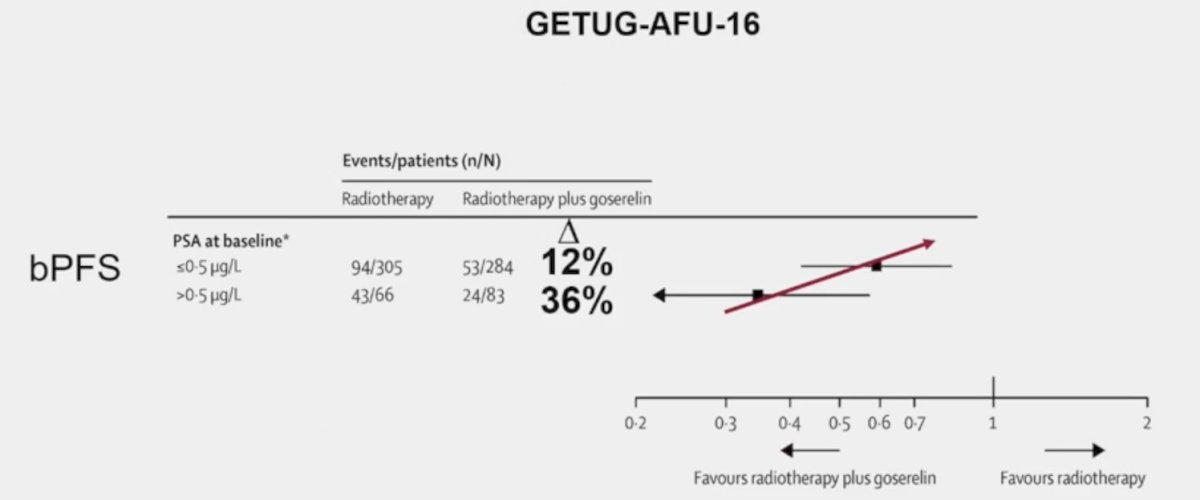
as well as SPPORT/RTOG 0534: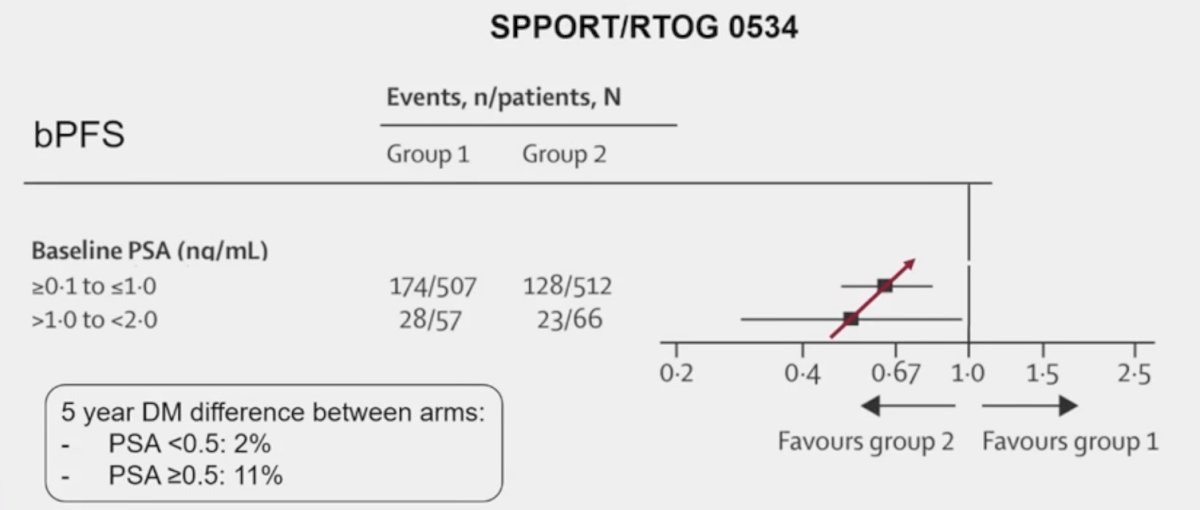
as well as RADICALS-HD: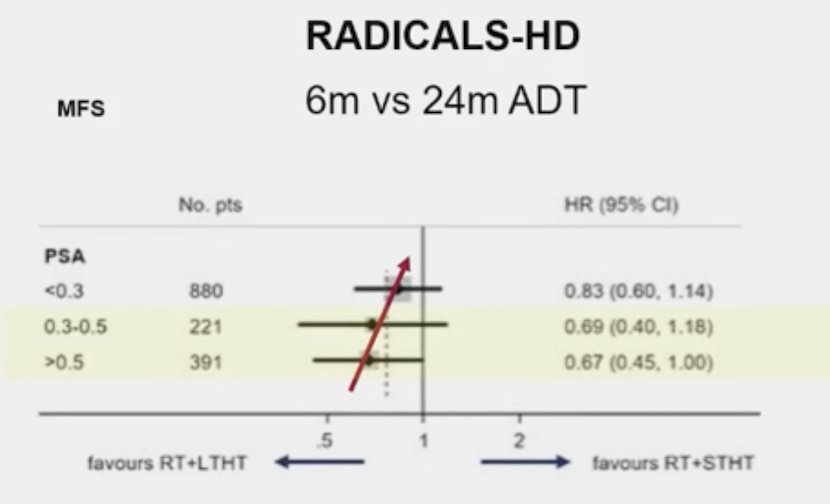
and for Formula-509: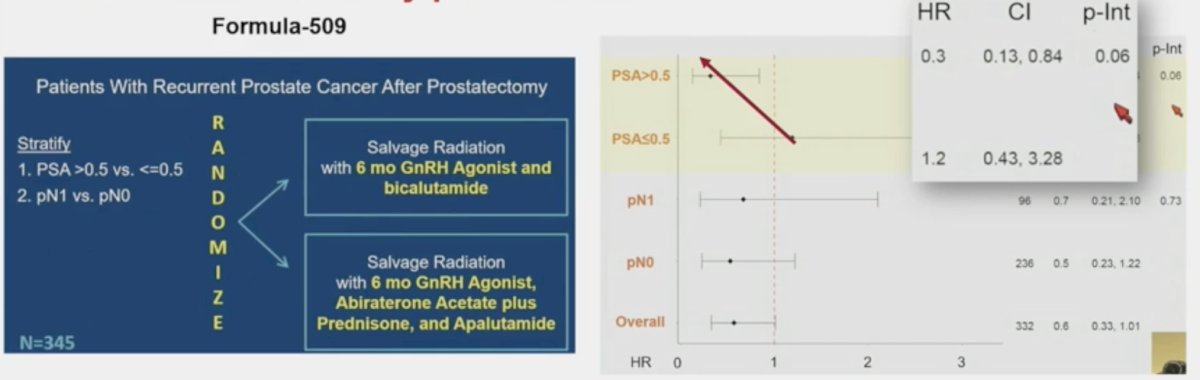
Dr. Spratt emphasized that the Decipher 22-gene genomic classifier also provides guidance in this disease space. Published in 2021 in JAMA Oncology,5 Feng and colleagues validated the Decipher genomic classifier in patients with recurrent prostate cancer using data from the RTOG 9601 randomized clinical trial. On multivariable analysis, the genomic classifier was independently associated with distant metastasis (HR 1.17, 95% CI 1.05-1.32; p = 0.006), prostate cancer-specific mortality (HR 1.39, 95% CI, 1.20-1.63; p < 0.001), and overall survival (HR 1.17, 95% CI 1.06-1.29; p = 0.002) after adjusting for age, race/ethnicity, Gleason score, T stage, margin status, entry PSA, and treatment arm. The cumulative incidence curve for prostate cancer-specific mortality is as follows (blue – low, yellow – intermediate, gray – high Decipher risk):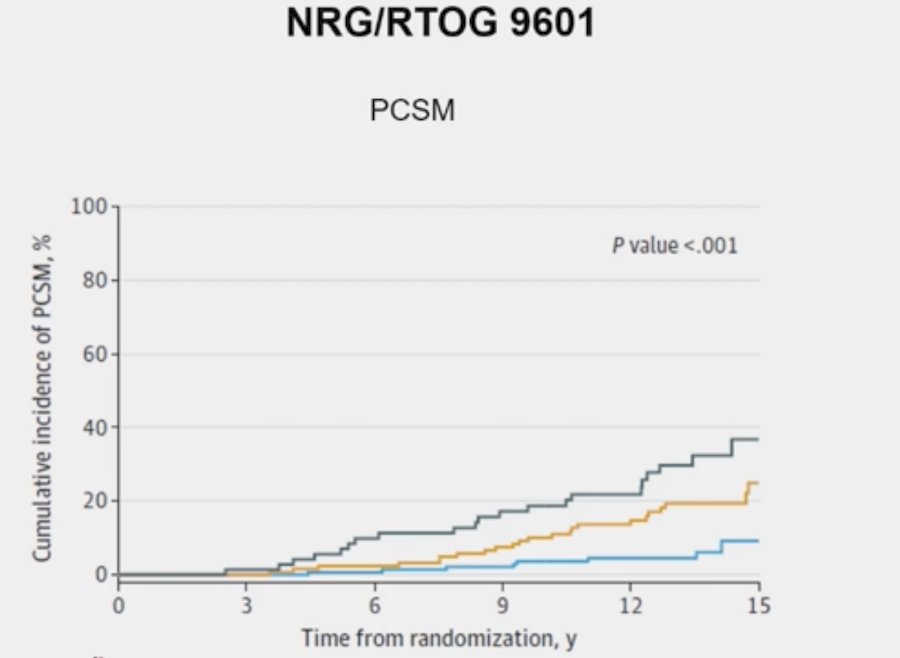
In the SAKK 09/10 trial (Swiss Group for Clinical Cancer Research), Dal Pra et al.6 conducted an analysis of 350 men with biochemical recurrence after radical prostatectomy who received salvage radiotherapy (64 – 70 Gy) without concurrent hormonal therapy or pelvic nodal radiotherapy. The primary endpoint was biochemical progression, whereas secondary endpoints were clinical progression and time to hormone therapy. The analytic cohort included 226 patients, with a median follow-up of 6.3 years. The Decipher genomic classifier score (high versus low-intermediate) was independently associated with the rates of biochemical progression (sHR 2.26, 95% CI 1.42 - 3.60; p < 0.001), clinical progression (HR 2.29, 95% CI 1.32 - 3.98; p = 0.003), and use of hormone therapy (sHR 2.99, 95% CI 1.55 - 5.76; p = 0.001). The Kaplan-Meier curve for freedom from hormonal therapy is as follows: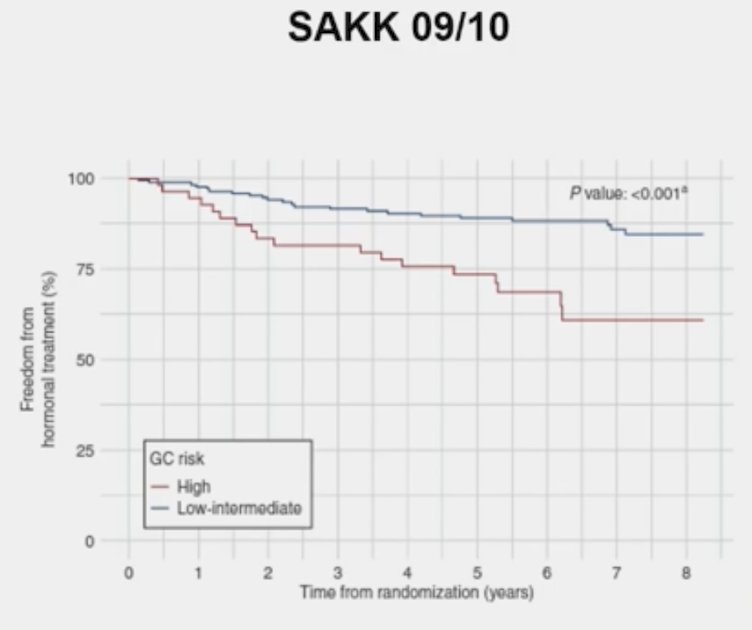
Dr. Spratt notes that at the upcoming AUA 2024 meeting, Dr. Todd Morgan will present results of “AI prognostic biomarker for recurrent prostate cancer after prostatectomy: Development and validation using deep learning on digital histopathology from NRG/RTOG-0534 and NRG/RTOG-0961,” the results of which we eagerly await.
Dr. Spratt concluded his presentation discussing what additional systemic therapy and duration of treatment are required for patients who receive salvage radiation therapy for biochemical recurrence with the following take-home messages:
- Hormone therapy has no clear overall survival benefit in unselected patients with early salvage radiotherapy
- This is different from localized prostate cancer with definitive radiotherapy
- Consistent with radiotherapy dose escalation improving outcomes in localized but not postoperative radiotherapy
- Signals of greater benefit from hormone therapy with salvage radiotherapy:
- High PSA (correlates with PSMA PET N+/M+)
- High 22-gene genomic classifier (correlates with PSMA PET N+)
Presented by: Daniel Spratt, MD, Chair and Professor of Radiation Oncology, UH Cleveland Medical Center, Seidman Cancer Center, Case Western Reserve University, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 Advanced Prostate Cancer Consensus Conference (APCCC) Meeting, Lugano, Switzerland, Thurs, Apr 25 - Sat, Apr 27, 2024.
Related content: Personalizing Salvage Radiation and Hormone Therapy for Biochemical Recurrence - Daniel Spratt
References:
- Shipley WU, Seiferheld W, Lukka HR, et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med 2017;376(5):417-428.
- Carrie C, Hasbini A, de Laroche G, et al. Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): A randomized, multicentre, open-label phase 3 trial. Lancet Oncol 2016;17(6):747-756.
- Pollack A, Karrison TG, Balogh AG, et al. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): An international, multicentre, randomized phase 3 trial. Lancet. 2022 May 14;399(10338):1886-1901.
- Dess RT, Sun Y, Jackson WC, et al. Association of presalvage radiotherapy PSA levels after prostatectomy with outcomes of long-term antiandrogen therapy in men with prostate cancer. JAMA Oncol. 202 May 1;6(5):735-743.
- Feng FY, Huang HC, Spratt DE, et al. Validation of a 22-Gene Genomic Classifier in Patients with Recurrent Prostate Cancer: An Ancillary Study of the NRG/RTOG 9601 Randomized Clinical Trial. JAMA Oncol. 2021 Apr 1;7(4):544-552.
- Dal Pra A, Ghadjar P, Hayoz S, et al. Validation of the Decipher genomic classifier in patients receiving salvage radiotherapy without hormone therapy after radical prostatectomy - an ancillary study of the SAKK 09/10 randomized clinical trial. Ann Oncol. 2022;33(9):950-958.
Related Content: