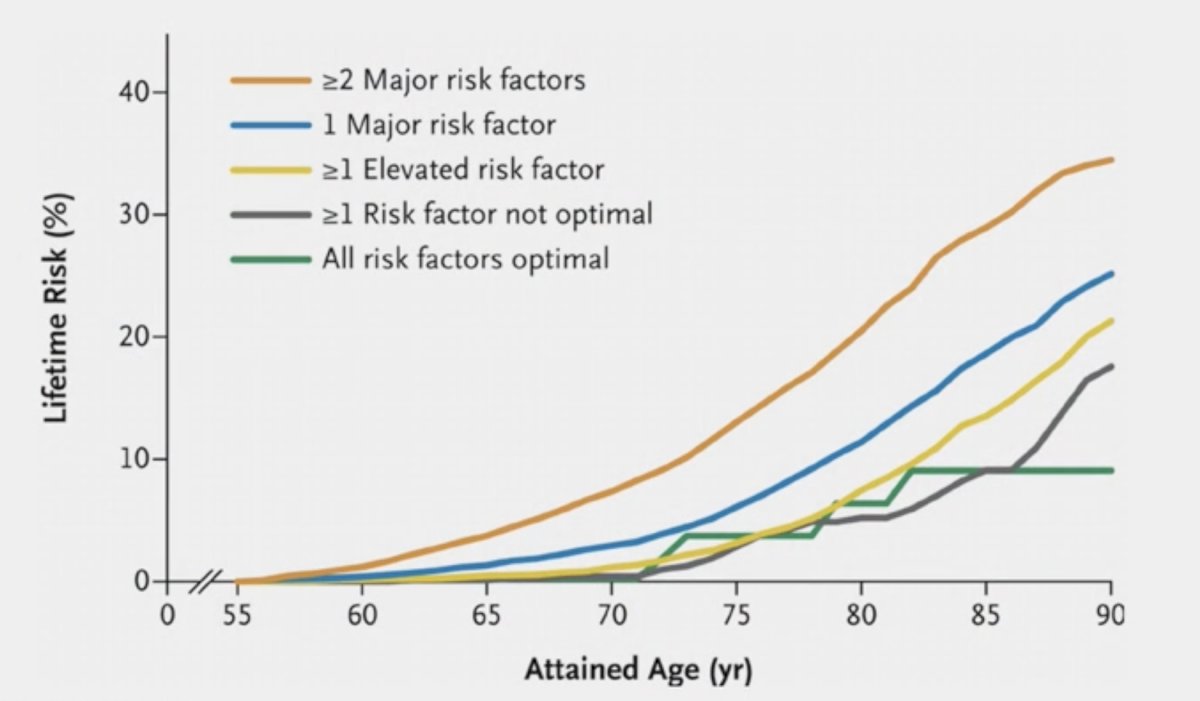
(UroToday.com) The 2024 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a session on the identification, assessment, and management of side effects of systemic therapies, and a presentation by Dr. Thomas Suter discussing how to prevent and monitor patients with cardiovascular complications in advanced prostate cancer. Dr. Suter started his presentation by emphasizing that the lifetime risk of cardiovascular disease significantly increases with more major risk factors, with a nearly 40% risk at 90 years of age for >= 2 major risk factors:
Systemic cancer therapy can have many cardiovascular side effects, including (i) hypertension, (ii) myocardial infarction, (iii) cardiac dysfunction, (iv) myocarditis, (v) arrhythmias, (vi) pulmonary hypertension, (vii) thromboembolism, and (viii) pleural effusion. Related to prostate cancer systemic therapy, Dr. Suter notes that the most common cardiovascular issues are related to hypertension, myocardial infarction, and cardiac dysfunction. Several prostate cancer specific therapies cause-specific cardiovascular issues, but the most common and important culprit (by far) is ADT: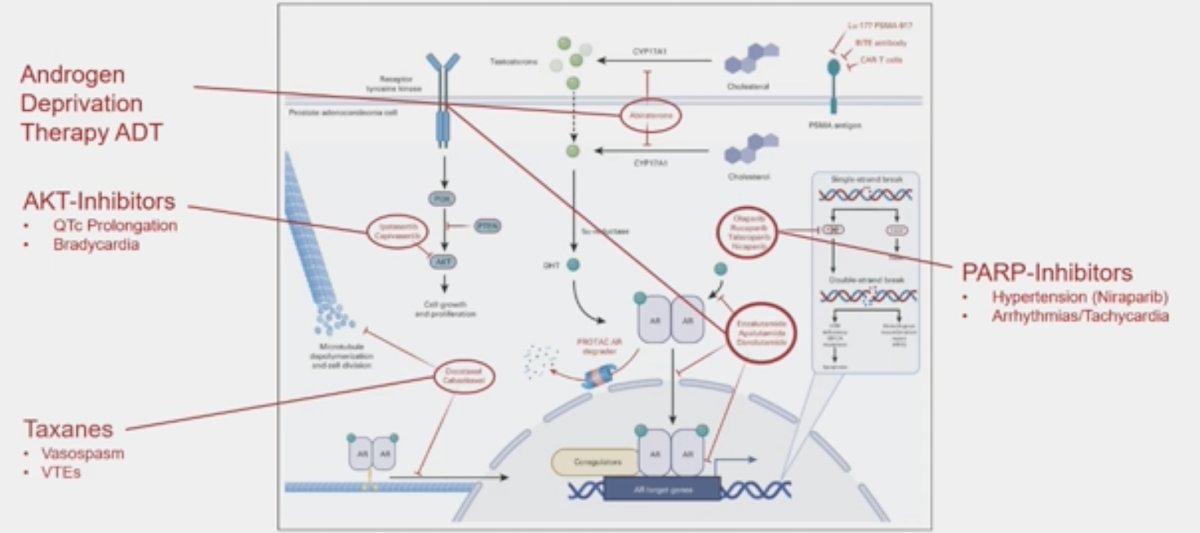
ADT appears to add insult to injury, exasperating general risk factors for cardiovascular morbidity, such as hypertension, dyslipidemia, diabetes, obesity, and physical inactivity: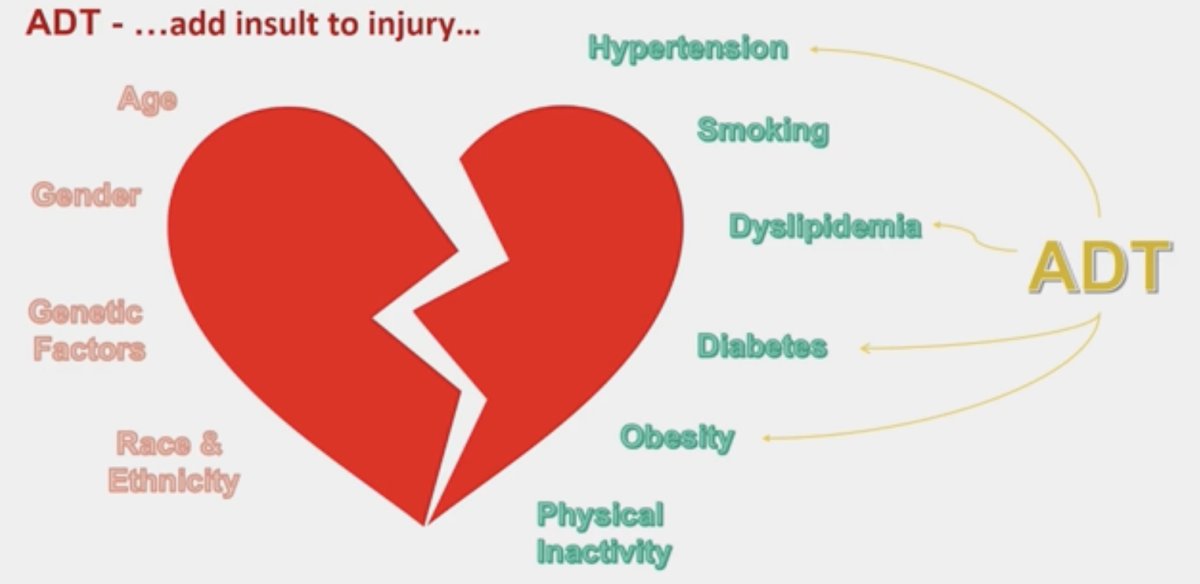
Androgen deprivation therapy-related cardiovascular toxicities for each specific treatment are outlined in the following figure:1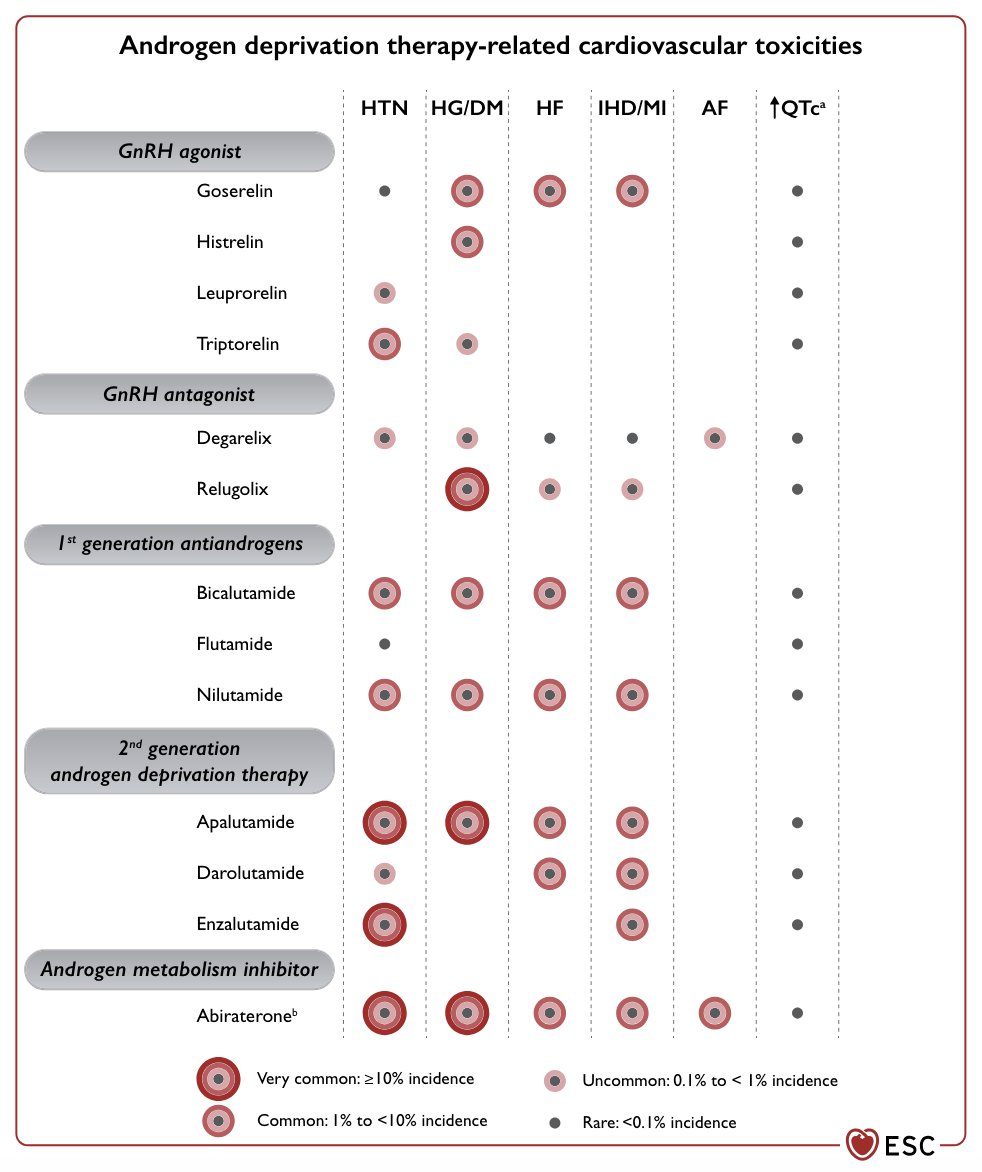
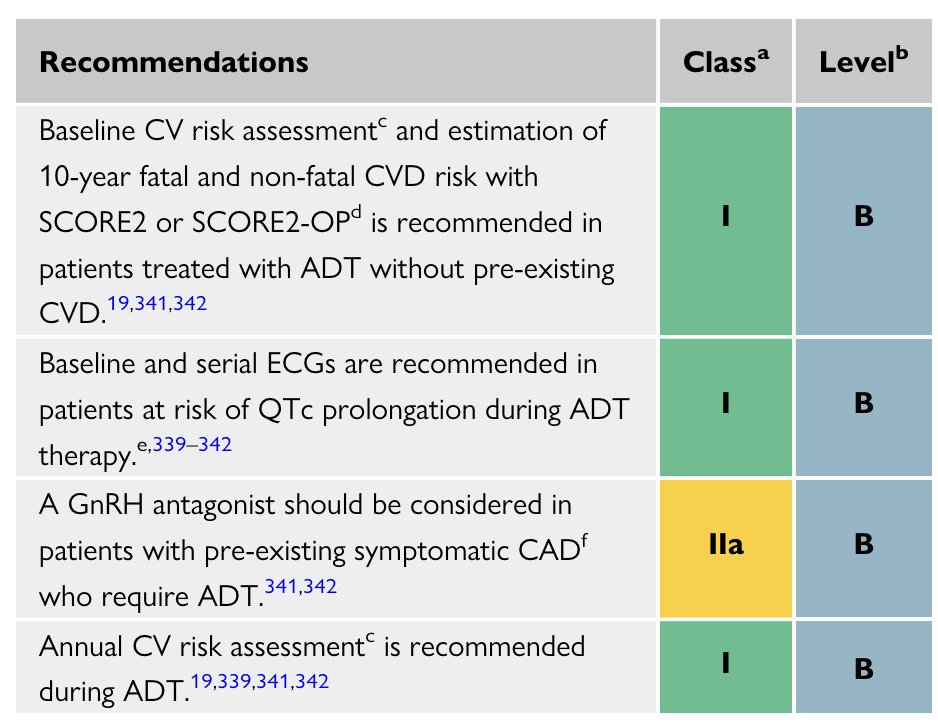
Recommendations for baseline cardiovascular risk assessment and monitoring during ADT for prostate cancer, include the following:1
- Baseline cardiovascular risk assessment and estimation of 10-year fatal and non-fatal cardiovascular risk (SCORE2 assessment)
- Baseline and serial EKGs are recommended in patients at risk of QTc prolongation during ADT therapy
- A GnRH antagonist should be considered in patients with pre-existing symptomatic coronary artery disease who require ADT
- Annual cardiovascular risk assessment is recommended during ADT
Hypertension monitoring is also important with the following metrics set as being “hypertensive” for patients on ADT:
- 24-hour average: >= 130/80 mm Hg (primary criterion)
- Daytime (awake) average: >= 135/85 mm Hg
- Night-time (asleep) average: >= 120/70 mm Hg
We also must monitor for heart failure as a complication of advanced prostate cancer treatment, which may be more challenging and relies on BNP levels and echocardiograms in patients with suspected heart failure.
Dr. Suter also discussed the RADICAL-PC analysis assessing the burden of uncontrolled cardiovascular risk factors in men with prostate cancer.2 Among 2,811 consecutive men (mean age 68 ± 8 years) with prostate cancer from Canada, Israel, Brazil, and Australia, the authors defined poor overall risk factor control as ≥3 of the following:
- Suboptimal low-density lipoprotein cholesterol (>2 mmol/L if Framingham Risk Score ≥15 and ≥3.5 mmol/L if Framingham Risk Score <15)
- Current smoker
- Physical inactivity (<600 MET min/week)
- Suboptimal blood pressure (≥140/90 mm Hg if no other risk factors, systolic blood pressure ≥120 mm Hg if known cardiovascular disease or Framingham Risk Score ≥15, and ≥130/80 mm Hg if diabetic)
- Waist: hip ratio >0.9
Overall, 99% had ≥1 uncontrolled cardiovascular risk factor, and 51% had poor overall risk factor control. Not taking a statin (OR 2.55, 95% CI 2.00-3.26), physical frailty (OR 2.37, 95% CI 1.51-3.71), need for blood pressure medications (OR 2.36, 95% CI 1.84-3.03), and age (OR per 10-year increase: 1.34, 95% CI 1.14-1.59) were associated with poor overall risk factor on multivariable logistic regression analysis:
Dr. Suter concluded his presentation discussing how to prevent and monitor patients with cardiovascular complications in advanced prostate cancer with the following take-home messages emphasizing several uncertainties:
- ADT has negative metabolic consequences and increased cardiovascular morbidity/mortality
- Current studies are not specifically designed to test cardiovascular outcomes
- There are no long-term studies
- Is there primary prevention effective?
- Is secondary prevention effective?
Presented by: Thomas Suter, MD, Bern University Hospital, University of Bern, Bern, Switzerland
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 Advanced Prostate Cancer Consensus Conference (APCCC) Meeting, Lugano, Switzerland, Thurs, Apr 25 - Sat, Apr 27, 2024.
References:
- Lyon AR, Lopez-Fernandez T, Couch LS, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO), and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022 Nov 1;43(41):4229-4361.
- Klimis H, Pinthus JH, Aghel N, et al. The Burden of Uncontrolled Cardiovascular Risk Factors in Men with Prostate Cancer: A RADICAL-PC Analysis. J Am Coll Cardiol CardioOnc. 2023 Feb;5(1):70-81.
Related Content: