He began by discussing the demographics of bladder and kidney cancer, emphasizing that these are predominately diseases of older adults. However, in spite of this, he demonstrated that older adults are dramatically under-represented in clinical trials. Further, there was little improvement between 2001 and 2011. Unfortunately, there haven’t been further improvements in the subsequent decade either.
He emphasized a number of barriers to enrollment of older adults to clinical trials, including systemic barriers, provider-related barriers, patient-related barriers, and caregiver-related barriers. Two overarching modifications which may address this include operational modifications to facilitate older patient enrollment including infrastructure as well as expanding the reach of the care of older adults with cancer beyond the trial sphere into routine clinical care.
He then highlighted data on older adults enrolled in pivotal clinical trials in metastatic bladder cancer. Based on a meta-analysis of phase II and phase III data of cisplatin-based combination chemotherapy, he emphasized the work of Dr. Matt Galsky demonstrating comparable results for septuagenarians as compared to their younger counterparts, with the caveat that all included patients were cisplatin-eligible. More recently, assessing the role of avelumab maintenance therapy following induction chemotherapy for advanced or metastatic urothelial carcinoma from the JAVELIN Bladder 100 study, he showed subgroup analyses showing benefit among older patients, with an even greater benefit in patients aged 65 years and older. Further, patients aged 65 years and older comprised 70% of this study cohort.
Moving to consider pivotal trials in kidney cancer, trials in both first-line and second-line therapy as of 2018 showed that patients who are older than 65 years derived just as much benefit from their as younger patients in terms of efficacy and, further, they were able to tolerate therapy. In the second-line setting, immunotherapy was similarly well tolerated by older adults who derived comparable benefits as younger patients.
The SIOG (International Society of Geriatric Oncology) has published position statements regarding the care of elderly patients with both metastatic renal cell carcinoma (last updated in 2018) and bladder cancer (published in 2020). He emphasized that one of the values of these position papers is the included algorithms, such as the one for metastatic renal cell carcinoma highlighted below.
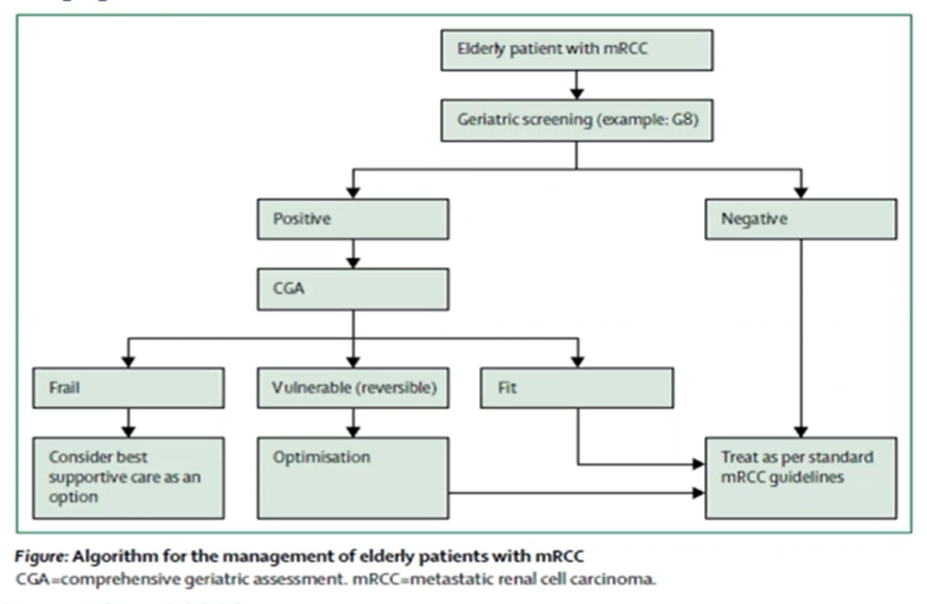
This algorithm emphasizes the importance of using a geriatric screen. For those patients who screen negative, they may be treated per standard recommendations. In contrast, those who screen positive should undergo a comprehensive geriatric assessment to determine their frailty and suitability for systemic therapy. For vulnerable patients, optimization may allow patients to receive standard of care oncologic treatment.
Dr. Kanesvaran then highlighted the G8 screening tool for geriatric assessment. This 8-question tool includes domains assessing cognition, function, falls, depression, nutrition, and comorbidity. This tool is useful given that a full geriatric assessment may take up to an hour.
He then highlighted the value of geriatric assessment and intervention. The GAP 70 study randomized patients with advanced cancer aged 70 years and older to receive a geriatric intervention or usual care. Those who received geriatric intervention had fewer toxicities and comparable overall survival. The GAIN study further demonstrated that geriatric intervention was associated with decreased treatment-related toxicity.
In summary, he concluded that older adults are under-represented in clinical trials generally though this appears to be less so in trials of systemic therapy in advanced kidney and bladder cancer. After a geriatric assessment, older adults can derive similar benefits from systemic therapies as their younger counterparts.
Presented by: Ravindran Kanesvaran, MD, Medical Oncologist, National Cancer Centre Singapore
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center Contact: @WallisCJD on Twitter at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021