To do so, the authors performed a systematic search of the literature encompassing the period January 2004-December 2020 using PubMed and clinical trials.gov to identify completed phase III trials in patients with mCRPC post-docetaxel. To be eligible for inclusion, trials had to be randomized phase III therapeutic trials that reported OS, PFS, or rPFS. In keeping with standard methodology, OS was measured from the date of random assignment to date of death from any cause or date of the last follow-up while rPFS was defined as the time from random assignment to date of disease progression on CT or bone scan per trial definition of death from any cause, whichever occurred first. PFS included PSA progression as a component of the composite endpoint. The authors assessed trial-level surrogacy by fitting linear regression on the treatment effect of rPFS (or PFS) and OS. It was pre-specified that rPFS would be considered a valid surrogate for OS if R² was 0.7 or higher.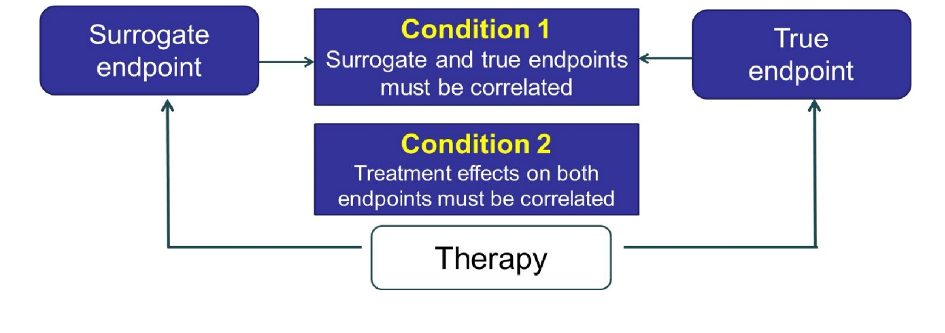
The authors identified 33 relevant trials in men with mCRPC post docetaxel approval of which 30 trials with 29,456 patients had data sufficient to allow assessment of the association between PFS and OS. Individual patient data were available from 12 trials and 11,941 patients.
In terms of condition 1, the authors found moderate correlation between the surrogate and true endpoints: among 11941 patients, the correlation between rPFS and OS was R2 = 0.61 (95 % CI = 0.60-0.63). Among 11,980 patients, the correlation between PFS and OS was R2 = 0.55 (95 % CI = 0.54-56).
The authors then assessed the condition that the treatment effects on both endpoints must be correlated.
At the trial level, the correlation between rPFS and OS was R2 = 0.50 (95 % CI = 0.39-0.70) while it was 0.53 (95 % CI = 0.38-0.67) for PFS and OS.
The authors conclude that, while this meta-analysis demonstrated a moderate correlation between treatment effects of rPFS and OS in patients with mCRPC, this correlation did meet the pre-specified surrogacy threshold of 0.7. Further, the correlation between PFS and OS was weaker than rPFS and OS.
Presented by: Susan Halabi, Ph.D., Duke Cancer Institute
Written by: Christopher J.D. Wallis, MD, Ph.D., Urologic Oncology Fellow, Vanderbilt University Medical Center, Contact: @WallisCJD on Twitter at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting #ASCO21, June, 4-8, 2021