(UroToday.com) At the 2022 American Society of Clinical Oncology Annual Meeting held in Chicago and virtually, the poster session focused on Kidney and Bladder cancers on Saturday afternoon included a presentation from Dr. Geraldine Pignot regarding the role of hyperthermic-intra-vesical chemotherapy as treatment for patients with BCG-refractory non-muscle invasive bladder cancer (NMIBC).
The majority of patients with newly diagnosed bladder cancer will have NMIBC. Among these, most will have low-grade, low-risk disease. However, those who are found to have higher risk disease at the time of TURBT are recommended to receive adjuvant intravesical Bacillus Calmette-Guérin (BCG) on the basis of decreased risks of recurrence. While BCG is efficacious, a significant proportion of patients with develop BCG refractory for whom the standard of care is radical cystectomy. Many patients may be unwilling or unable to undergo cystectomy, and as such there is a significant unmet need to identify alternative intravesical therapies to minimize the risk of recurrence and progression. One such approach is chemohyperthermia by HIVEC (Hyperthermic-Intra-Vesical Chemotherapy) which the authors assessed in this abstract.
From June 2016 to September 2021, the authors prospectively accured patients treated with HIVEC (6 weekly instillations) for BCG-refractory NMIBC. While all of these patients had a theoretical indication for cystectomy, they were ineligible for surgery or refused it. The primary study endpoint was 1-year recurrence-free survival (RFS) with secondary endpoints including 6-month complete response rate for carcinoma in situ (CIS), 1-year overall and cancer-specific survival rates and bladder preservation rate.
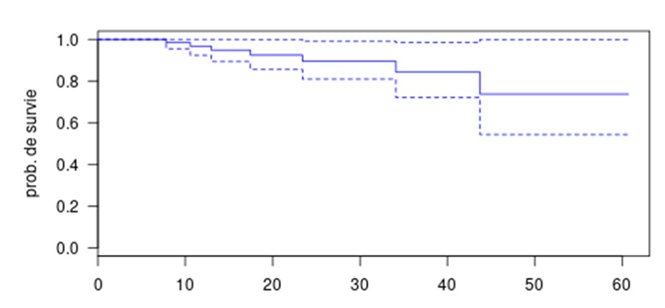
The authors enrolled 70 patients who were treated consecutively. The mean age of included patients was age 70 [42-89] years. After a mean follow-up of 19.7 months, 35 patients recurred (mean time of 10.6 months) and 8 patients eventually underwent cystectomy. The recurrence-free survival rate was 62.3% at 1 year and 40.2% at 2 years.

Eight patients progressed to a muscle-invasive disease, after a mean delay of 6.7 months. Five of these patients subsequently experienced metastatic progression and died from bladder cancer. Cancer-specific and overall survival rates were 95.1% and 92.9% at 1 year, and 87.5% and 77.8% at 2 years.
The bladder preservation rate was 90%. Among patients with CIS (34% of the cohort), the 6-month complete response rate was 75%. The presence of CIS was not a predictive factor of response to HIVEC. Tolerance was excellent with 38.2% grade 1-2 adverse events and no grade 3-4 adverse events.
Thus, the authors conclude that chemohyperthermia using the HIVEC device achieved a RFS rate of 53.1% at 1 year and enabled a bladder preservation rate of 90%. While cystectomy remains the standard of care for patients with BCG-refractory NIMBC, HIVEC may be discussed cautiously for patients who are not eligible for surgery and well informed of the risk of progression to muscle-invasive disease.
Presented by: Geraldine Pignot, MD, Institut Paoli-Calmettes, Marseille, France