(UroToday.com) The 2023 ASCO annual meeting included a session on doublet or triplet therapy for metastatic renal cell carcinoma (RCC), featuring a presentation by Dr. Naomi Haas discussing factors that influence decision-making. Dr. Haas started her presentation by highlighting two case presentations. The first patient was a 61-year-old male who works full time, is a runner, has an ECOG performance score of 0, and has a medical history of hypertension on an ACE inhibitor who presented with anemia (Hgb 10.0 g/dL). He was subsequently diagnosed with a large renal mass (biopsied clear cell RCC) with pulmonary nodules and a solitary liver metastases. The treatment options provided by Dr. Haas are as follows:
- VEGFR-TKI + IO (doublet)
- CTLA4 inhibitor + immune checkpoint inhibitor (doublet)
- Triplet (VEGFR-TKI + CTLA4 inhibitor + immune checkpoint inhibitor)
The second patient was a 79-year-old female, retired, with an ECOG performance status of 1 (fatigue and osteoarthritis in the knees and hands) who presented with a Hgb of 10.0 g/dL, and a large renal mass biopsied clear cell RCC with metastases to the lungs and liver (solitary metastases). Again, the treatment options provided by Dr. Haas are as follows:
- VEGFR-TKI + IO (doublet)
- CTLA4 inhibitor + immune checkpoint inhibitor (doublet)
- Triplet (VEGFR-TKI + CTLA4 inhibitor + immune checkpoint inhibitor)
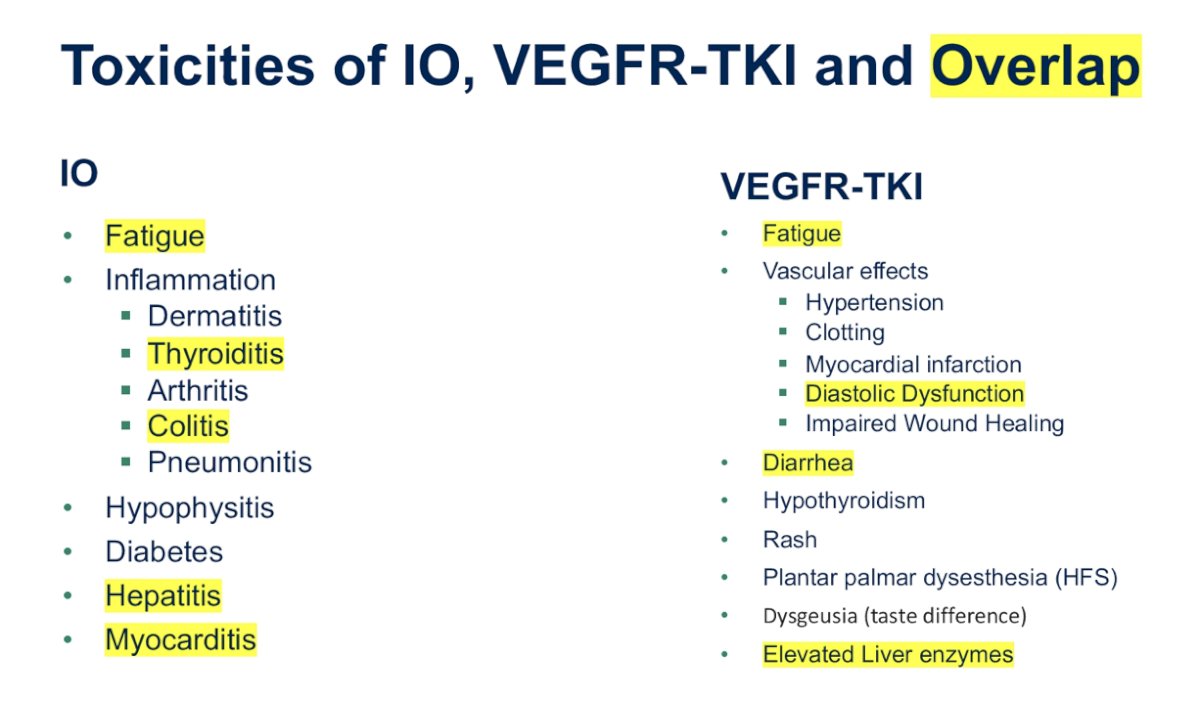
Dr. Haas notes that there are several factors to consider for these patients: (i) toxicities of treatment, (ii) health related quality of life, (iii) secondary measures of clinical efficacy including response rates and primary progressive disease rates, and (iv) clinicopathologic factors or biomarkers that might enrich response to treatment. Dr. Haas then provided the following summary of toxicities of immunotherapy, VEGFR-TKI, and highlighted those that overlap:
Indeed, therapy can be toxic and intolerable for these patients. Grade 1 and 2 side effects are not routinely reported in publications as not “unsafe”. Even grade 1 and 2 adverse events are intolerable over a long period of time. Dr. Haas then provided several clinical tools available to help with assessing patients:
- Karnofsky or ECOG performance status
- IMDC favorable, intermediate or poor risk
- Health related quality of life measured using the FKSI-19 domains (physical disease-related symptoms, emotional disease related symptoms, treatment side effects, and functional well being)
- DepOR-percentage of a tumor shrinkage correlating with clinical outcomes in a number of solid tumors
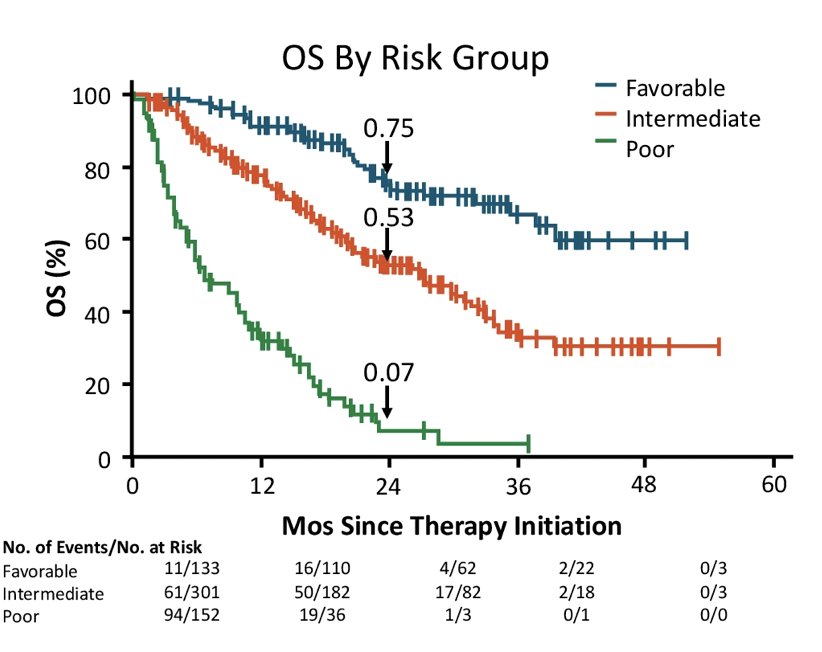
With regards to understanding the role of risk in the treatment of metastatic RCC, the IMDC criteria for metastatic RCC has been around since 2009:1
- Karnofsky performance score <80%
- Time from initial diagnosis to targeted treatment < 1 year
- Hemoglobin < lower limit of normal
- Calcium > 10mg/dL
- Platelet count > upper limit of normal
- Neutrophil count > upper limit of normal
Favorable risk: 0 risk factors; intermediate risk: 1-2 risk factors; poor risk: 3+ risk factors
There are also promising biologic tools, including PD-L1 expression, tissue-based transcriptome analysis, distinct biological clusters (angiogenesis, immune, cell cycle, metabolism, stromal programs), and liquid biopsies (circulating tumor DNA, cell-free DNA, circulating noncoding RNA). Additionally, there are important immunotherapy endpoints to consider, such as:
- Landmark progression free survival, overall survival, and duration of response
- Time to initiation of subsequent therapy
- Treatment-free survival, remission, and functional cure
- Overall quality of life and overall value
Dr. Haas concluded her presentation discussing factors that influence decision-making with the following take-home points:
- Triplet therapy may eventually be optimal for some patients, but data is still emerging
- Treatment toxicities and patient health are important considerations
- Immune mediate response rates are useful for IO based trials
- Clinicopathologic factors (ie. health-related quality of life, depth of response, IMDC criteria) or biomarkers (ie. transcriptomics, cell free material) could help better identify ideal populations for doublet or triplet therapy
Presented by: Naomi B. Haas, MD, University of Pennsylvania-Abramson Cancer Center, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.
References:
- Heng DY, Xie W, Regan MM, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: Results from a large, multicenter study. J Clin Oncol. 2009 Dec 1;27(34):5794-5799.