(UroToday.com) The 2023 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL between June 2nd and June 6th was host to a prostate, testicular, and penile cancers oral abstract session. Dr. Alberto Bossi presented late-breaking results from the phase III PEACE-1 trial evaluating prostate irradiation in men with de novo, low-volume, metastatic castrate-sensitive prostate cancer (mCSPC).
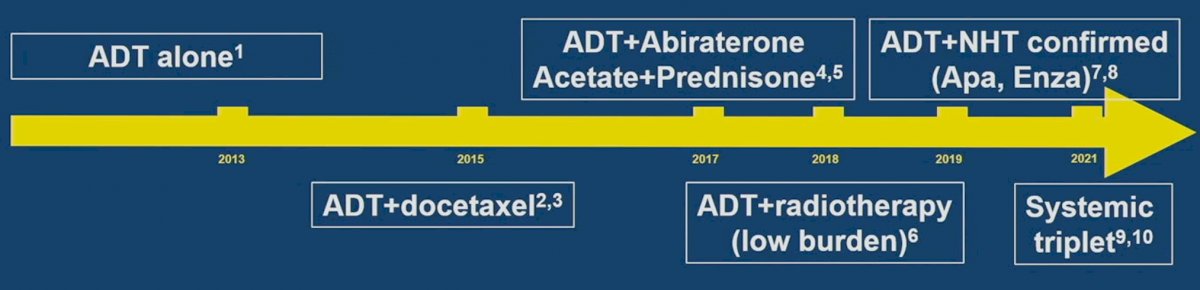
The treatment landscape of mCSPC patients has evolved considerably over the last decade, as demonstrated in the figure below:
The PEACE Consortium (Prostate Cancer Consortium in Europe) is an academic European program that aims to conduct phase 3 trials for men with prostate cancer. This is a flexible structure that requires at least two European countries to be involved. Each trial can be sponsored by any academic hospital, and each trial is independent.
The PEACE-1 trial was sponsored by Unicancer, and seven countries contributed to its accrual. Eligible patients had de novo mCSPC and could have received up to 3 months of ADT prior to randomization. Patients were stratified by metastatic site, performance status, type of testosterone lowering therapy, and the use of docetaxel. A total of 1173 men were randomized 1:1:1:1 as shown below. Standardized treatments included continuous ADT or bilateral orchiectomy, with or without docetaxel at 75 mg/m2 every three weeks for six cycles, plus recommended G-CSF. Abiraterone treatment consisted of 1000 mg/day with prednisone 5 mg twice per day until disease progression or intolerance and was administered along with docetaxel for patients who underwent chemotherapy. Radiotherapy to the prostate was delivered in 37 fractions for a cumulative dose of 74 Gy after patients completed docetaxel, if receiving chemotherapy.
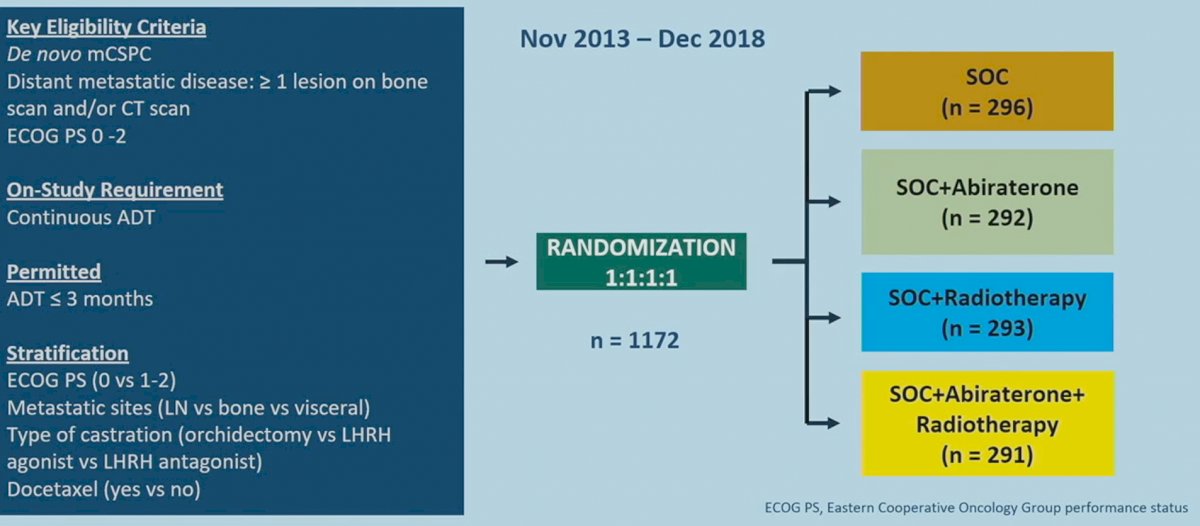
Various amendments were implemented during the course of the trial due to the evolving standard of care in this disease. After 2015, docetaxel was permitted as part of the standard of care per investigator’s discretion and patient consent. After LATITUDE and STAMPEDE were reported, it became unethical to administer ADT alone, and so docetaxel administration (without abiraterone) was made mandatory.
The two co-primary endpoints of the study were radiographic progression-free survival (rPFS) and overall survival. The trial used a 2 x 2 factorial design aimed at answering two questions, the role of abiraterone and the role of radiotherapy on top of the standard of care (SOC). This trial has previously demonstrated that addition of abiraterone to SOC (i.e., abiraterone + ADT +/- docetaxel +/- radiotherapy) was associated with rPFS (HR: 0.54, 95% CI: 0.41-0.71, p<0.0001) and OS improvements (HR: 0.82, 95% CI: 0.69 – 0.98, p=0.03).1
In this report, Dr. Bossi presented the results of the analysis of the efficacy and safety of prostate radiotherapy for patients with low volume, de novo mCSPC. The co-primary endpoints for this analysis were OS and rPFS, assessed per the Prostate Cancer Working Group 2 (PCWG2) criteria and with imaging performed at least every 6 months following a rising PSA. Numerous other secondary endpoints were assessed, with a particular focus on:
- Castrate resistance-free survival
- Serious genitourinary event-free survival
- Toxicity
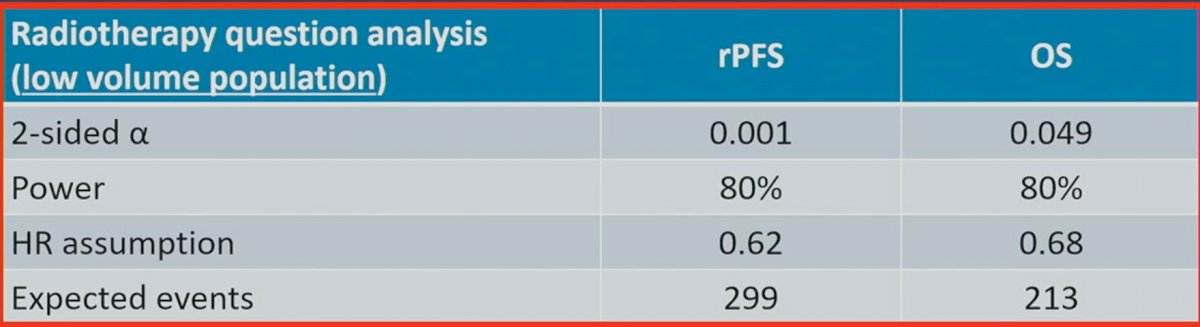
From a trial design and statistical planning perspective, Dr. Bossi noted that the “alpha spending” (i.e., the false positive rate) of 0.05 was split between the rPFS (0.001) and OS (0.049) outcomes.
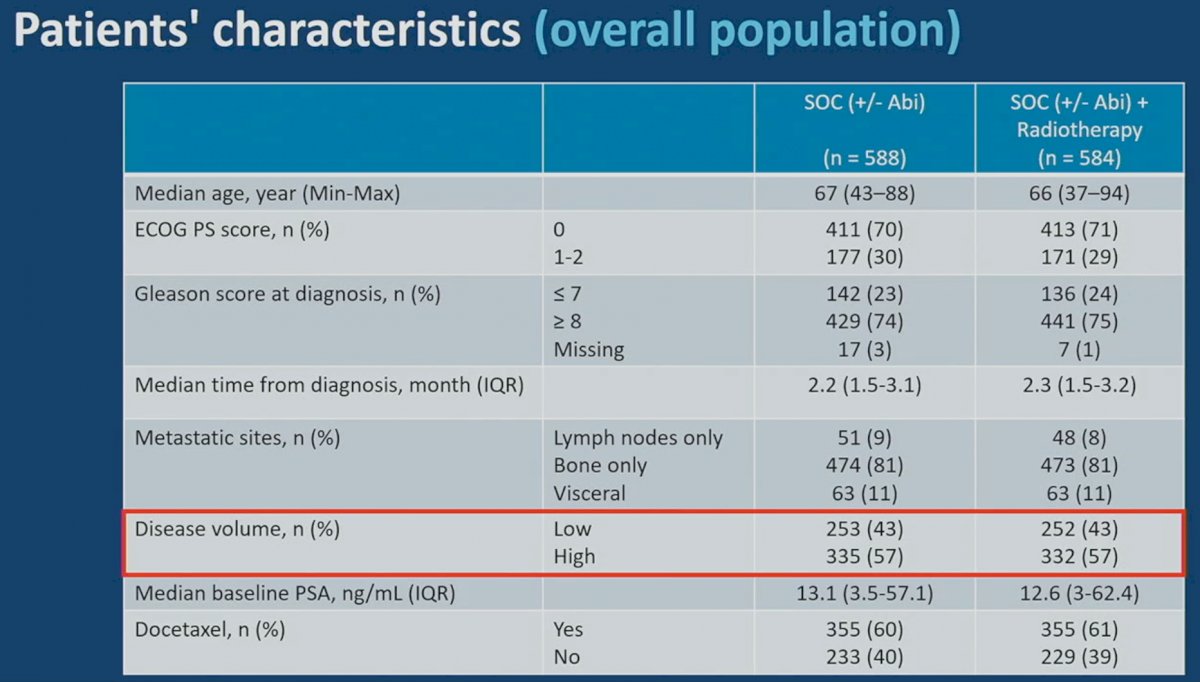
There were no significant differences in baseline characteristics between the two treatment arms of XRT + SOC +/- abiraterone and SOC +/- abiraterone. Of note, 43% of patients in each arm had low-volume disease. The median baseline PSA was 12.6 – 13.1 and 60% had received prior docetaxel.
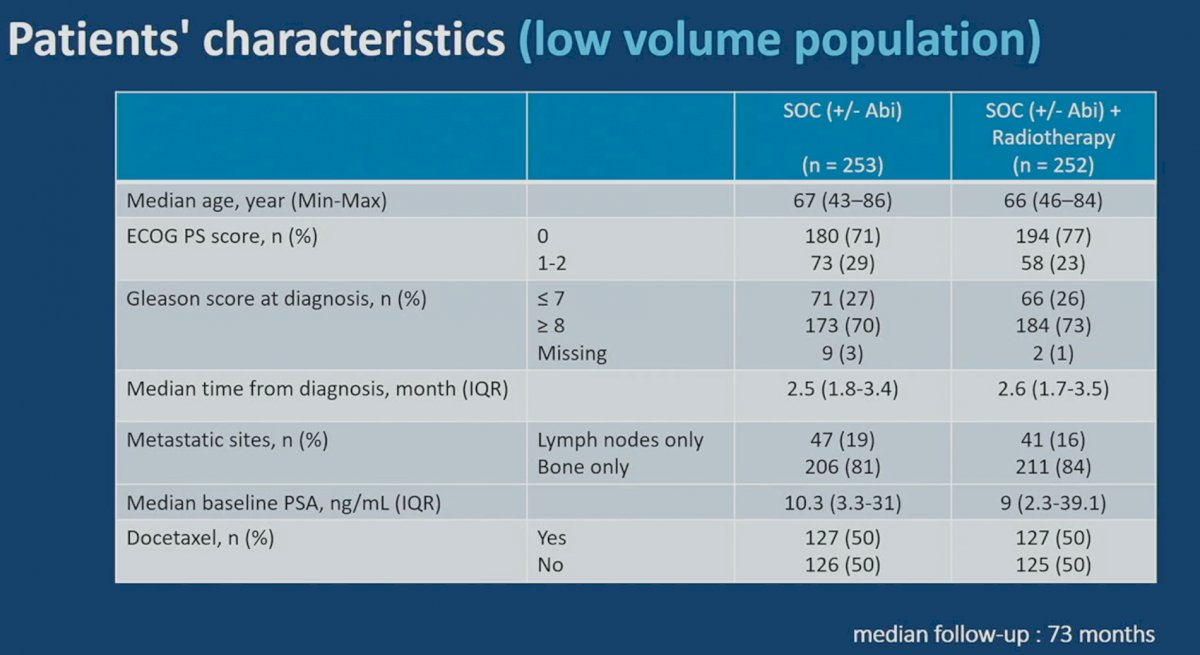
When evaluating the target population of low-volume patients specifically, there were similarly no significant differences in baseline characteristics, stratified by receipt of radiotherapy (yes/no). 50% of patients in this low-volume cohort had received docetaxel. The median follow-up was 73 months.
For the rPFS outcome, a qualitative interaction between radiotherapy and abiraterone was observed (p=0.026), and, given this, each of the four experimental arms were assessed individually. Conversely for OS, the pre-defined threshold for statistical interaction was not reached (p=0.12), and thus the two radiotherapy arms (XRT + SOC and XRT + SOC + abiraterone) were pooled for this analysis.
Dr. Bossi first presented the rPFS outcomes in the low volume population, stratified by the treatment arm. As demonstrated below, addition of prostate radiotherapy to SOC + abiraterone was associated with significant rPFS benefits (median 7.5 versus 4.4 years, p=0.02). Conversely, addition of radiotherapy to SOC alone was not associated with rPFS benefits (median 2.6 versus 3.0 years; HR: 1.11, 95% CI: 0.67 – 1.84, p=0.61).

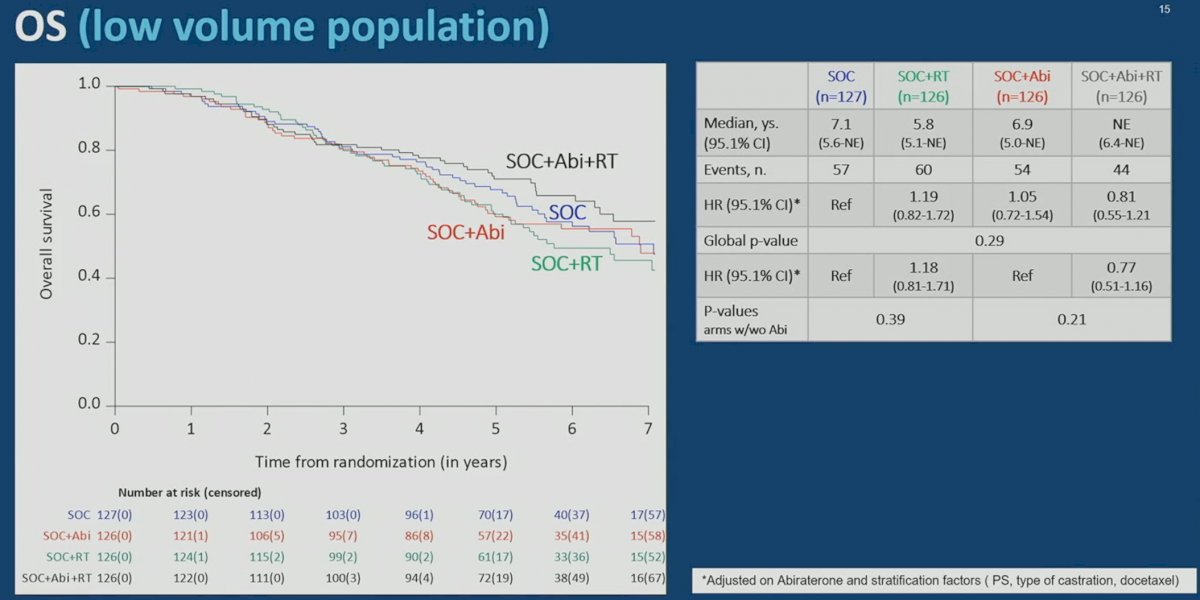
The addition of prostate radiotherapy to either SOC alone or SOC + abiraterone was not associated with OS improvements. In the SOC + abiraterone arms, addition of prostate radiotherapy was associated modest, non-significant OS benefits (HR: 0.77 , 95% CI: 0.51 – 1.16, p=0.21). Similarly, addition of prostate radiotherapy to SOC alone did not improve OS (HR: 1.18, 95% CI: 0.81- 1.71, p=0.39).
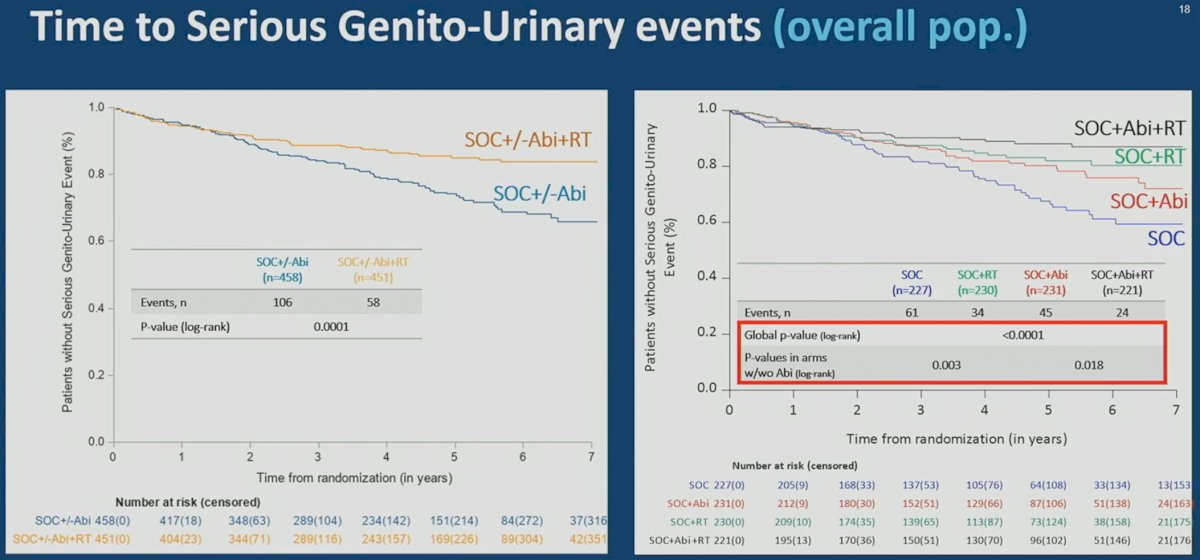
Interestingly, addition of prostate radiotherapy to SOC +/- abiraterone in the low-volume cohort was associated with significant improvements in the time to serious genitourinary events (p=0.0006). This overall benefit was consistent irrespective of whether patients had prostate radiotherapy added to SOC + abiraterone (p=0.003) or SOC alone (p=0.048). A similar benefit was observed in the overall cohort (p=0.001).

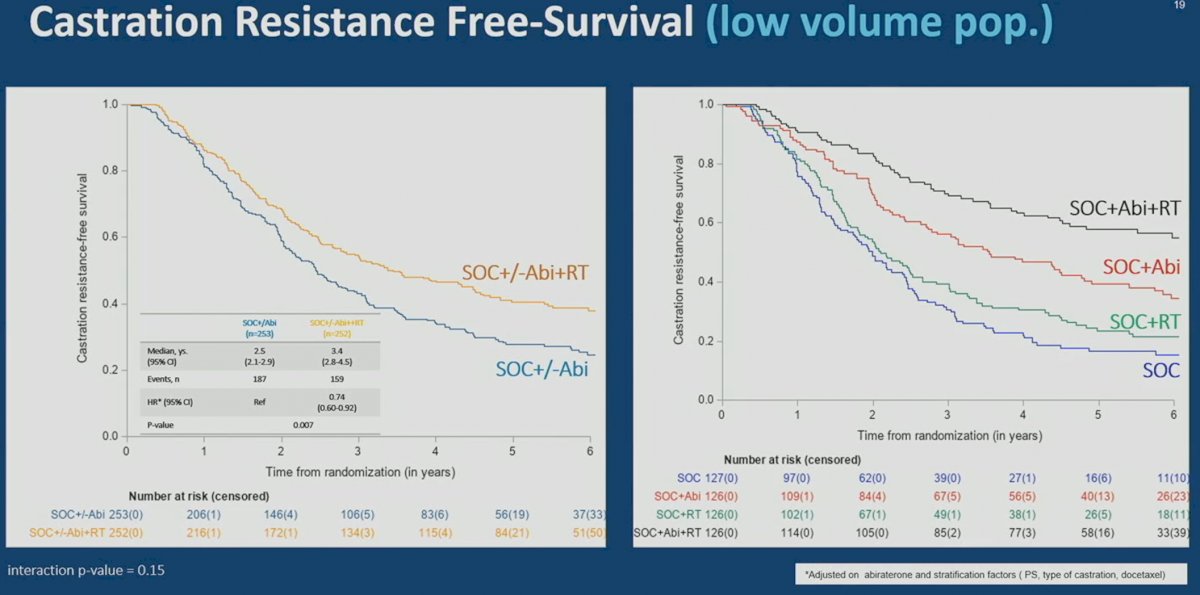
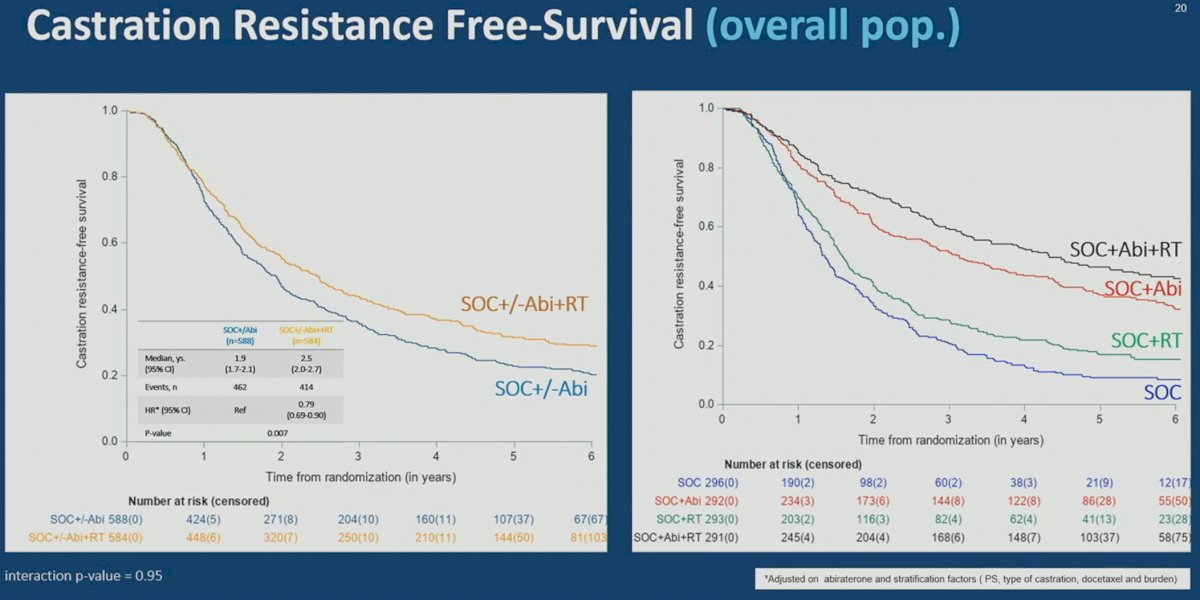
A similar pattern was observed for castration resistance free-survival, whereby addition of prostate radiotherapy to SOC + abiraterone or SOC alone was associated with significant improvements in the low-volume (median 3.4 versus 2.5 years; HR: 0.74, 95% CI: 0.60 – 0.92, p=0.007) and overall cohorts (median: 2.5 versus 1.9 years; HR: 0.79, 95% CI: 0.69 – 0.90, p=0.007).
A similar toxicity profile was observed among patients receiving radiotherapy versus not, as summarized below:
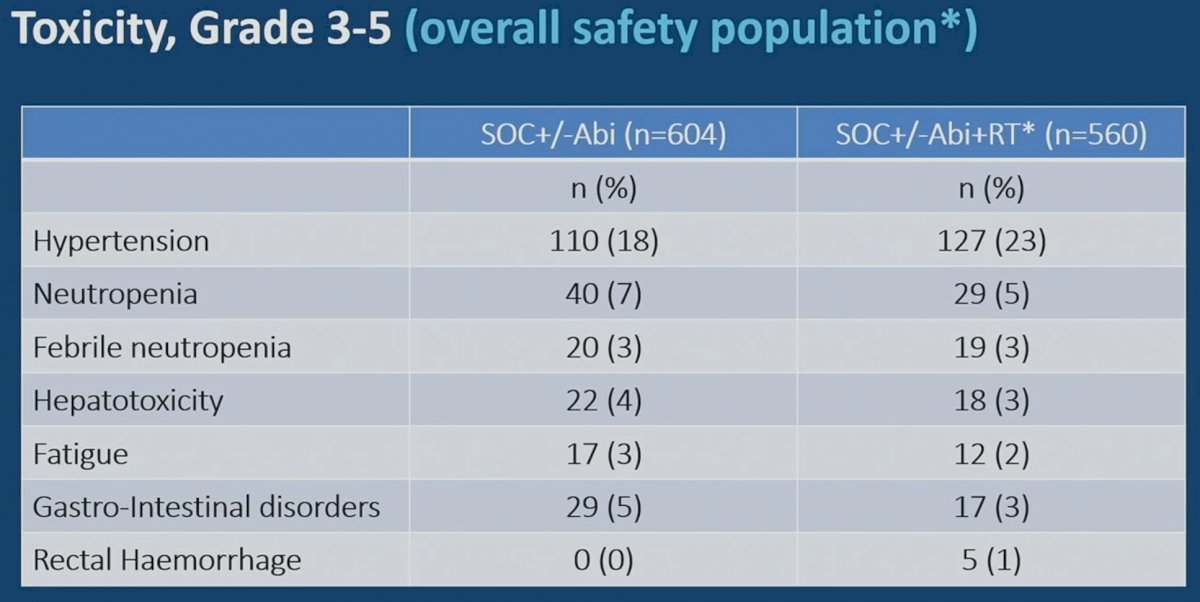
Dr. Bossi concluded that combining prostate radiotherapy with intensified systemic treatment (abiraterone +/- docetaxel) was associated with improved rPFS and CRPC free-survivals in men with low volume, de novo mCSPC. To date, it does not appear that prostate radiotherapy improves OS in such men, albeit with minimal added toxicity. Interestingly, it appears that the addition of prostate radiotherapy in this setting is associated with improvements in the rates of serious GU events, irrespective of the metastatic burden.
Presented by: Alberto Bossi, MD, Professor, Head of the Urology and Prostate Brachytherapy Unit, Department of Radiation Oncology, Institute Gustave Roussy, Paris, France
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.
References:
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.