(UroToday.com) The 2023 ASCO annual meeting included a session on the management of prostate cancer in older adults, featuring a presentation by Dr. Ravi Parikh discussing known and novel intervention strategies for helping our elders survive and thrive with prostate cancer. Dr. Parikh started by noting that the “frailty phenotype” in prostate cancer is as follows:
- Weakness
- Slowness
- Low physical activity
- Exhaustion
- Unintentional weight gain (or weight loss)
Furthermore, prostate cancer and its therapy can exacerbate frailty, leading to inactivity, slowing and weakening, and falls, dysfunction, and disability: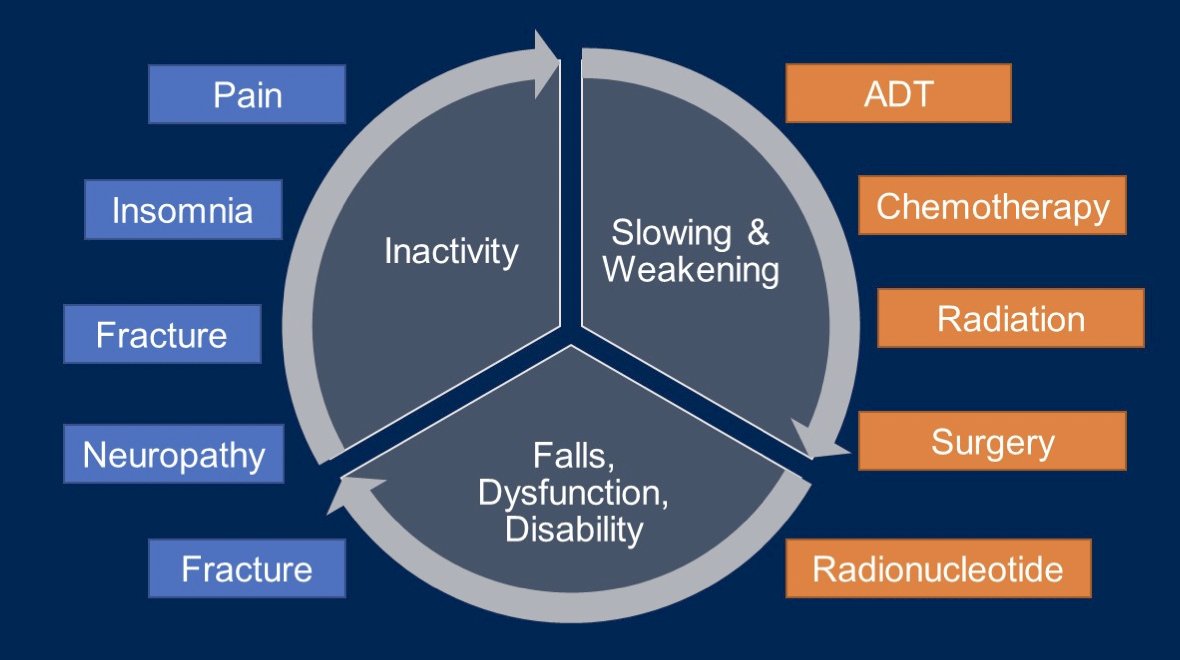
With regards to frailty in prostatectomy patients, 1 in 7 patients undergoing prostatectomy are considered frail. For those undergoing surgery, frailty is associated with:
- 2x the rate of major complications
- Twice as long length of stay
- $3,160 greater total health costs per admission
One way to mitigate frailty for those undergoing surgery is prehabilitation, which improves wellbeing throughout the cancer continuum:
Components of prehabilitation may include (i) aerobic exercise programs, (ii) weight-bearing exercise, (iii) pelvic floor exercises, (iv) psychological counselling, (v) sexual counselling, (vi) fruit and vegetable rich diet, and (vii) replacing red meat. Shinall and colleagues previously showed the association of preoperative patient frailty and operative stress with postoperative mortality.1 Among 432 828 unique patients, 36 579 (8.5%) were frail and 9113 (2.1%) were very frail. The 30-day mortality rate among patients who were frail and underwent the lowest-stress surgical procedures (ie cystoscopy) was 1.55%, and among patients with frailty who underwent the moderate-stress surgical procedures (ie. laparoscopic cholecystectomy) was 5.13%. For those patients who were very frail, 30-day mortality rates were higher after the lowest-stress surgical procedures (10.34%) and after the moderate-stress surgical procedures (18.74%).
For patients with prostate cancer undergoing ADT, the frailty phenotype may be as high as 40%. Frailty mitigation for these patients is of the utmost importance and should include nutritional optimization, exercise, physical therapy, and strength training. Treatment selection should also be considered: (i) for those at risk of falls, careful consideration should be placed when prescribing abiraterone, darolutamide, enzalutamide and apalutamide; (ii) for those at increased cardiovascular risk, relugolix should be used instead of leuprolide.
Additionally, ADT accelerates bone loss and is associated with a 10-20% risk of significant fracture at 5 years. ADT associated fractures decrease quality of life and functional status, and may increase prostate cancer related mortality by 40%. Guidelines suggest that baseline and periodic assessment of bone mineral density via DEXA scans and calculation of the World Health Organization Fracture Risk Assessment Tool (FRAX) score (prior to ADT) are recommended. Ways to improve bone health include supplementation of calcium and vitamin D (usually >= 600 U), tobacco cessation, weight-bearing exercises, and use of bone targeted agents. For castrate sensitive disease, no anti-resorptive therapy is necessary unless the patient is high-risk:
- T-score <= 2.5
- Major osteoporotic fracture >= 20%
- Hip fracture >= 3%
- A history of hip or vertebral fracture (the patient should receive weekly alendronate, annual IV Zometa, q6 month denosumab, and continual screening for secondary causes of poor bone health)
For castrate resistant disease, anti-resorptive therapy is indicated, either with bisphosphonates or denosumab q12 weeks.
Dr. Parikh noted that biomechanical computed tomography (CT) is an opportunity for assessment of bone health. Key advantages of this technology are the opportunistic capture of bone strength from routine CTs, and measurement of multiple metrics for assessing fracture risk: bone strength, bone mass, etc: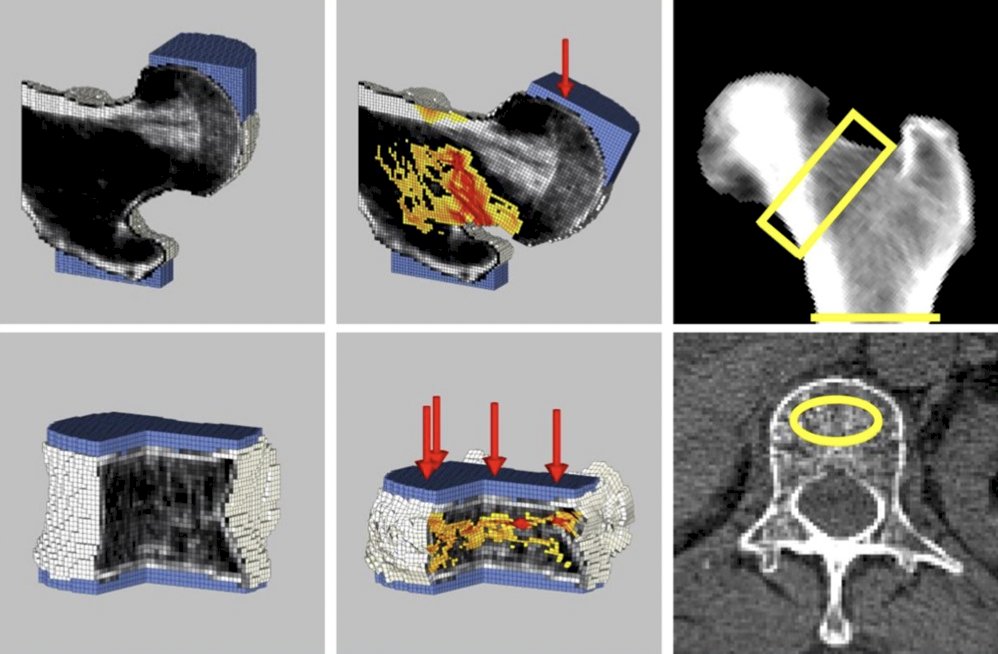
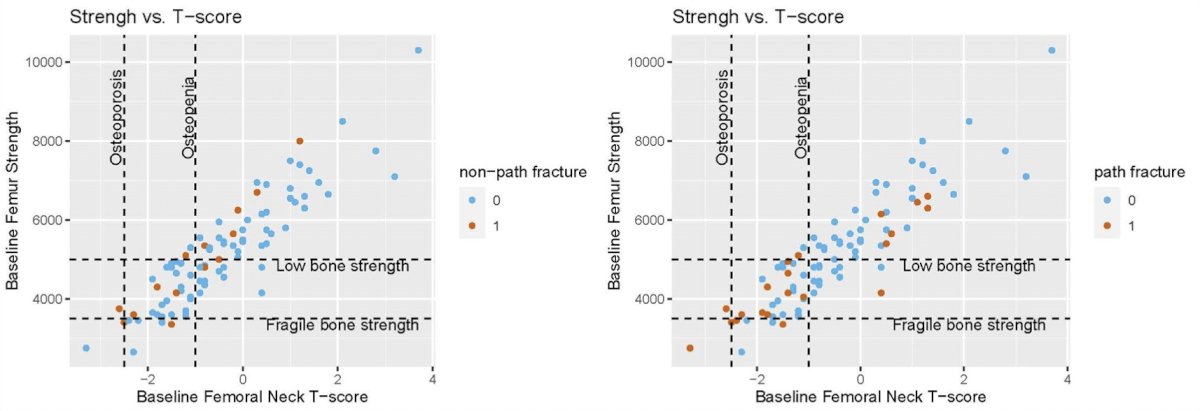
Furthermore, biomechanical CT has been shown to be strongly correlated with DEXA scan imaging and fracture risk: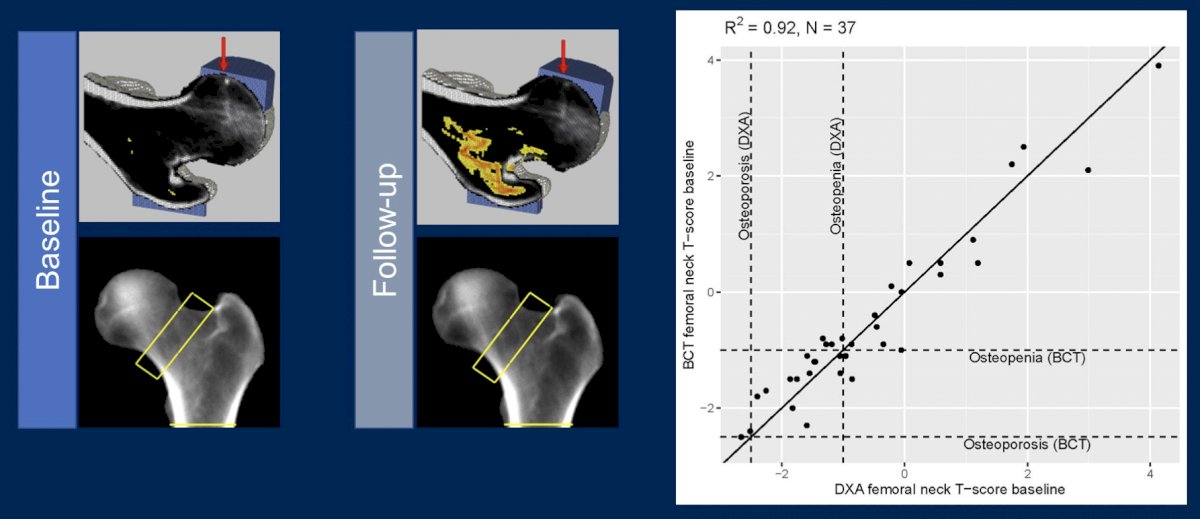
Dr. Parikh concluded his presentation discussing known and novel intervention strategies for helping our elders survive and thrive with prostate cancer with the following take-home points:
- Frailty is prevalent among prostate cancer survivors, particularly among individuals who are peri-surgery and/or on ADT
- Prehabilitation and treatment modification based on frailty assessment can improve peri-surgical outcomes
- Clinical trials to test impacts of functional balance, strength, or mobility programs will inform management of patients on ADT
- Risk-based assessment to direct antiresorptive therapy utilization is standard-of-care in non-castrate resistance prostate cancer, but is limited by reliance on DEXA. Biomechanical CT and other radiomics techniques are opportunities for continued advancement
Presented by: Ravi Bharat Parikh, MD, MPP, FACP, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, June 2 – Tues, June 6, 2023.
References:
- Shinall Jr MC, Arya S, Youk A, et al. Association of preoperative patient frailty and operative stress with postoperative mortality. JAMA Surg. 2020 Jan 1;155(1):e194620.