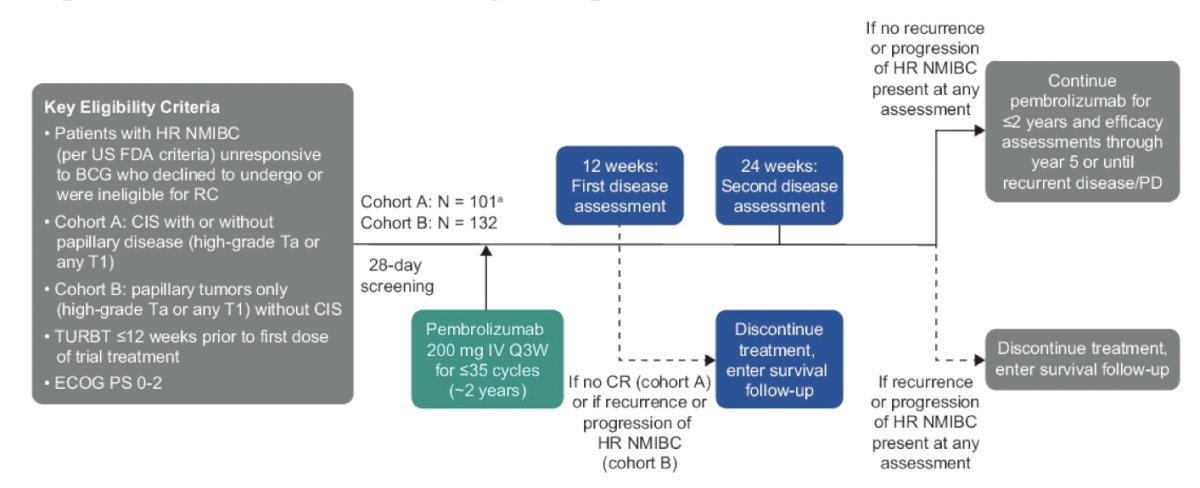
(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) annual meeting featured a session on bladder cancer, and a presentation by Dr. Roger Li discussing a post hoc analysis of KEYNOTE-057 assessing outcomes of patients with BCG–unresponsive high-risk non–muscle-invasive bladder cancer who demonstrated nonresponse to pembrolizumab. The phase 2 KEYNOTE-057 trial previously demonstrated that pembrolizumab can serve as a bladder-sparing option for patients with high-risk non–muscle-invasive bladder cancer who are unresponsive to BCG and are unable or unwilling to undergo radical cystectomy.1 In Cohort A, the primary endpoint of 3-month complete response rate was 40.6%, and for Cohort B, the primary endpoint of 12-month disease free survival rate was 43.5%. However, the outcomes (especially related to progressive disease) of patients who do not respond to bladder-sparing therapies, including pembrolizumab, are of concern. Dr. Li and colleagues conducted a post hoc analysis of the KEYNOTE-057 trial to assess the clinical outcomes of patients who experienced persistent or recurrent high-risk non–muscle-invasive bladder cancer despite pembrolizumab therapy and subsequently received either radical cystectomy or other bladder-sparing therapies (pooled analysis of cohorts A and B).
The KEYNOTE-057 study design is as follows:
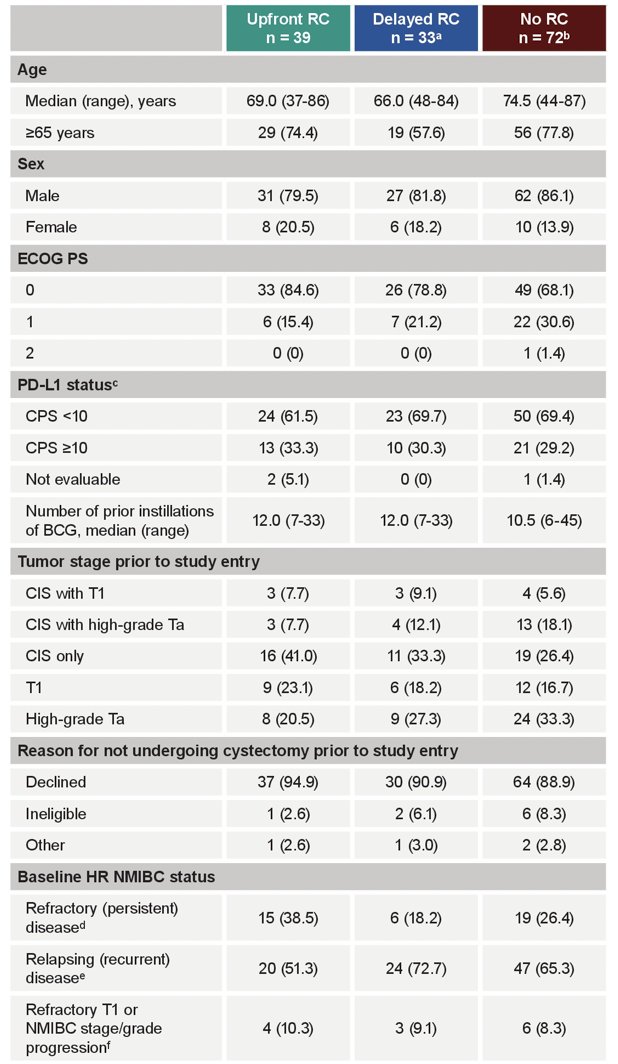
Patients with BCG-unresponsive CIS and/or papillary-only tumors who had nonresponse (persistent or recurrent high-risk non–muscle-invasive bladder cancer) to pembrolizumab were evaluated in the following groups:
- Patients who received upfront radical cystectomy (≤4 months of treatment failure confirmation)
- Patients who received delayed radical cystectomy (>4 months after treatment failure or received other bladder-sparing therapies before radical cystectomy)
- Patients who received bladder-sparing therapies alone (received bladder-sparing therapy alone or no reported subsequent treatment)
Analyses included progression free survival (lack of development of muscle-invasive bladder cancer or metastatic disease or death due to progressive disease) and overall survival, indexed from the date of pembrolizumab nonresponse. Patients with upfront radical cystectomy found to have upstaging to muscle-invasive bladder cancer (due to initial understaging) were excluded from the progression free survival analysis unless they developed subsequent progressive disease. Pathologic outcomes in patients undergoing upfront versus delayed radical cystectomy were also evaluated.
Among the 144 patients who were non-responders to pembrolizumab, the median time from pembrolizumab nonresponse to data cutoffs (cohort A: May 30, 2023; cohort B: Oct 20, 2022) was 59.7 months (range: 10.9-80.7). Among these patients, 39 underwent upfront radical cystectomy, 33 underwent delayed radical cystectomy, and 72 underwent bladder-sparing therapies alone:
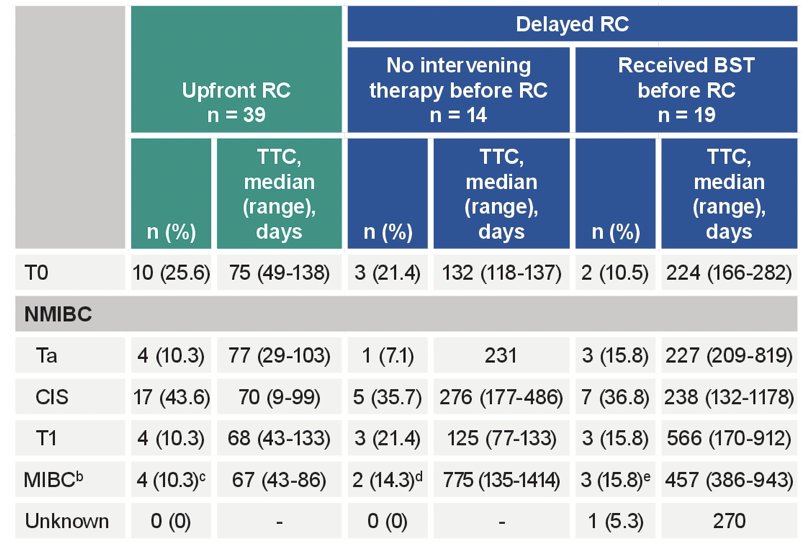
Of the patients who underwent upfront radical cystectomy, the pathologic stages were:
- T0: 26%
- Non–muscle-invasive bladder cancer (Ta, T1, CIS): 64%
- Muscle-invasive bladder cancer (T2, T3, T4): 10%
Of patients who underwent delayed radical cystectomy, the pathologic stages were:
- T0: 15%
- Non–muscle-invasive bladder cancer: 67%
- Muscle-invasive bladder cancer: 15%
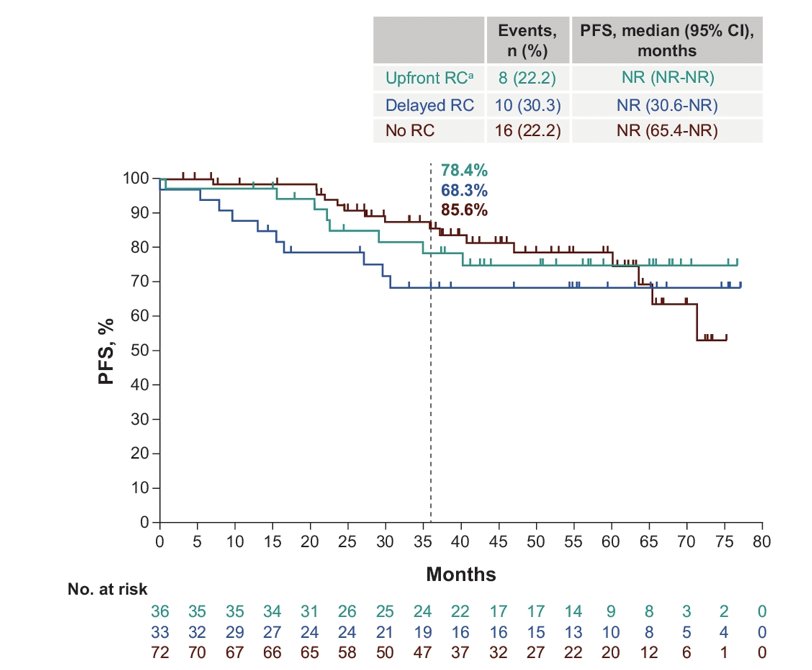
The median progression free survival was not reached across all three groups. The 36-month progression free survival rates were 78% (95% CI, 60-89) for upfront radical cystectomy, 68% (95% CI, 49-82) for delayed radical cystectomy, and 86% (95% CI, 74-92) for bladder-sparing therapy alone:
The median overall survival was not reached across all three groups:
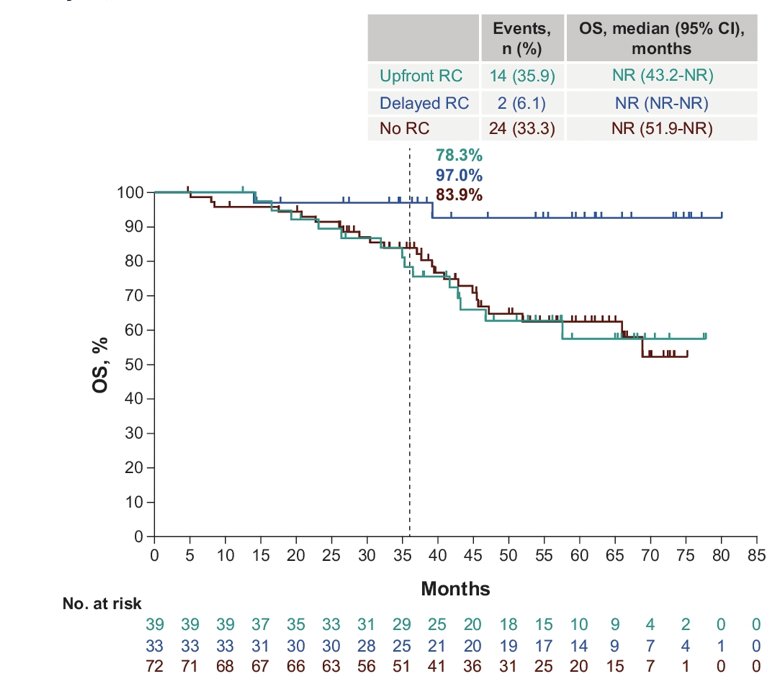
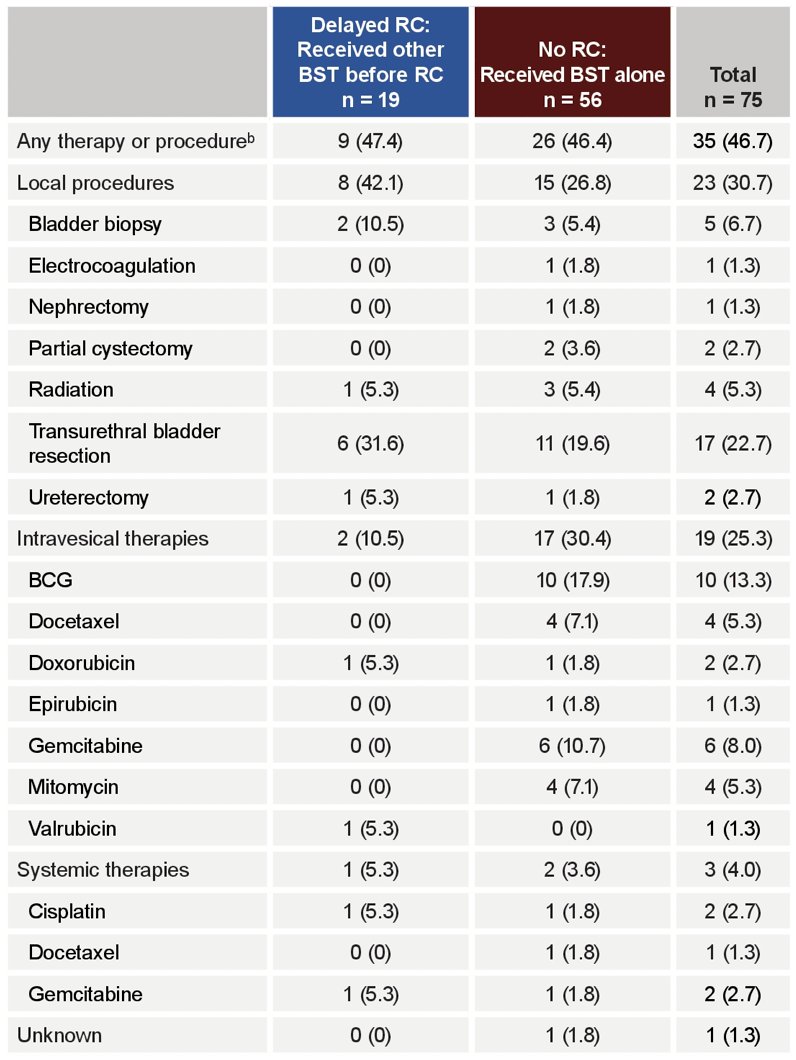
The subsequent therapies (other than radical cystectomy) after nonresponse to pembrolizumab in patients who underwent delayed radical cystectomy or who received bladder sparing therapy is as follows:
Dr. Li concluded his presentation by discussing a post hoc analysis of KEYNOTE-057 assessing outcomes of patients with BCG–unresponsive high-risk non–muscle-invasive bladder cancer who demonstrated nonresponse to pembrolizumab with the following take home messages:
- Oncologic outcomes were similar between patients treated with bladder-sparing therapies or radical cystectomy following nonresponse to pembrolizumab
- Patients who underwent upfront versus delayed radical cystectomy had similar pathologic outcomes
- Data from this analysis suggest that patients were not harmed by bladder-sparing therapies following pembrolizumab and that a window of safety may exist for implementing second-line bladder-sparing therapy prior to radical cystectomy
- The presented data can help patients and their physicians with further treatment decisions and deliver relevant information for the design of future clinical trials
Presented by: Roger Li, MD, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL between May 31st and June 4th
References: