(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL between May 31 and June 4 featured the Poster Session: Genitourinary Cancer: Prostate, Testicular, and Penile. Dr. Allison Thompson presented a Matched-adjusted indirect comparison (MAICs) of talazoparib plus enzalutamide (TALA+ENZA) versus olaparib plus abiraterone and prednisone/prednisolone (OLAP+AAP) for first-line therapy in patients with metastatic castration-resistant prostate cancer (mCRPC) and homologous recombination repair mutations (HRRm)/BRCAm.
Poly-ADP ribose polymerase inhibitors (PARPi) exploit the concept of synthetic lethality by targeting cells with deficiencies in homologous recombination repair (HRR), particularly those harboring mutations in genes such as BRCA1 and BRCA2. By inhibiting PARP, the cells' ability to repair DNA damage is compromised, resulting in genomic instability and ultimately cell death, thereby demonstrating therapeutic efficacy in prostate cancer patients with HRR pathway alterations.1
PARPi in combination with novel hormonal therapy (NHT) has shown benefit for the first-line treatment of mCRPC. Clinical trials, such as TALAPRO-22 (NCT03395197) and PROpel3 (NCT03732820), have shown the efficacy of PARPi+NHT, in all comers but particularly in patients with HRRm and BRCAm mutations.
To date, head-to-head randomized studies comparing PARPi+NHT combinations in the first-line setting of mCRPC are lacking and their comparative efficacy is unknown. The investigators used unanchored matching adjusted indirect comparison (MAIC), which provides a method to reweight patients, potentially accounting for cross-study differences. They made comparisons in these subpopulations (HRRm and BRCAm) for radiographic progression-free survival (rPFS) based on blinded independent central review (BICR) and overall survival (OS) across TALA+ENZA (TALAPRO-2) and OLAP+AAP (PROpel).
They utilized individual patient data from TALAPRO-2 Cohort 2 with a data cutoff of March 10, 2022 (rPFS/OS), and published summary-level data from PROpel with data cutoffs of July 30, 2021 (rPFS) and October 12, 2022 (OS).
To ensure consistency between the two trials, patients from TALAPRO-2 with specific HRRm/BRCAm (either co-occurring or standalone) that were not evaluated in PROpel were excluded from the dataset for each analysis. Furthermore, to better align populations TALAPRO-2 patients were matched based on PROpel's eligibility criteria, and their characteristics were adjusted to account for key prognostic factors identified in the literature and clinical expertise. These factors included prior taxane chemotherapy in castration-sensitive prostate cancer (CSPC), presence of visceral or bone-only metastasis, Eastern Cooperative Oncology Group (ECOG) score, prostate-specific antigen (PSA) levels, Gleason score, BRCA1, and BRCA2 mutation status. They used effective sample size (ESS) and standardized mean difference (SMD) to show the degree of overlap and population differences, respectively, between the adjusted TALA+ENZA and OLAP+AAP populations.
After excluding patients with specific gene mutations not assessed in PROpel and those who received prior novel hormonal therapy in CSPC, there were 157 and 64 patients remaining in the TALA+ENZA arm for HRRm and BRCAm, respectively. After reweighting, the resulting ESS was reduced by 14%.
Using unanchored MAIC, the primary analysis of rPFS showed better results with TALA+ENZA compared to OLAP+AAP (HR [95% CI]: 0.668 [0.429, 1.041]; p = 0.074) in the HRRm population. However, this was not statistically significant, and sensitivity and exploratory analysis adjusting for BRCA1/2 mutated patients were consistent with the primary analysis.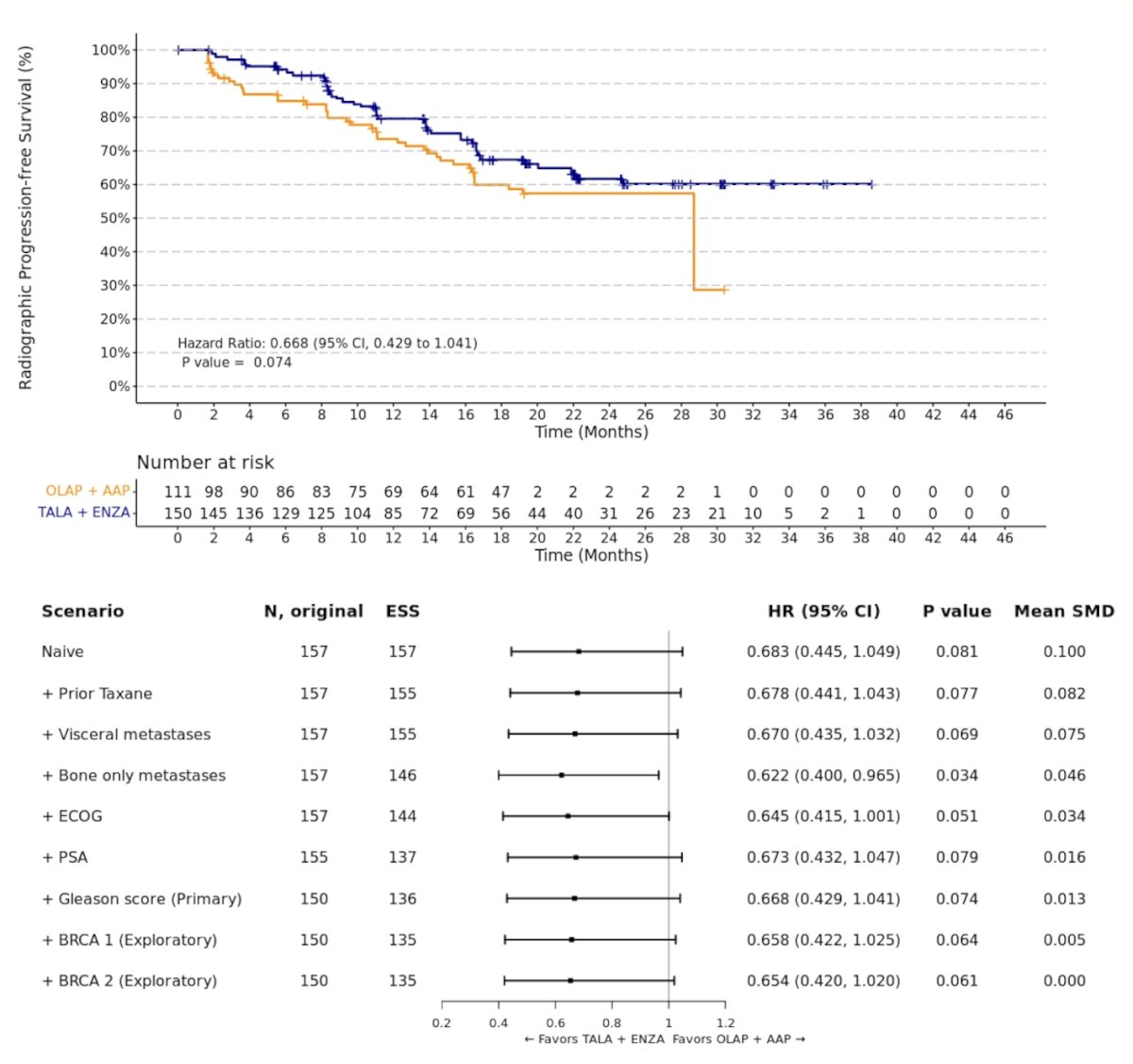
Similarly, the MAIC analysis of OS showed numerically better results with TALA+ENZA versus OLAP+AAP (HR [95% CI]: 0.663 [0.406, 1.082]; p = 0.100) in the HRRm population, but this was not significant and once again sensitivity and exploratory analysis adjusting for BRCA1/2 patients were consistent.
![the MAIC analysis of OS showed numerically better results with TALA+ENZA versus OLAP+AAP (HR [95% CI]: 0.663 [0.406, 1.082]; p = 0.100) in the HRRm population, but this was not significant and once again sensitivity and exploratory analysis adjusting for BRCA1/2 patients were consistent](/images/com-doc-importer/164-asco-2024/asco-2024-matching-adjusted-indirect-comparisons-of-talazoparib-plus-enzalutamide-versus-olaparib-plus-abiraterone-and-prednisolone-for-first-line-therapy-in-patients-with-mcrpc-and-hrr-mutations-brcam/image-1.jpg)
In the BRCAm population, both the rPFS and OS analyses showed no statistically significant differences between TALA+ENZA compared to OLAP+AAP (HR 0.824, p = 0.658 for rPFS) and (HR 1.014, p = 0.977 for OS). Exploratory and sensitivity analyses were consistent with the primary results in the BRCAm population. rPFS and OS curves are depicted in the graphics below.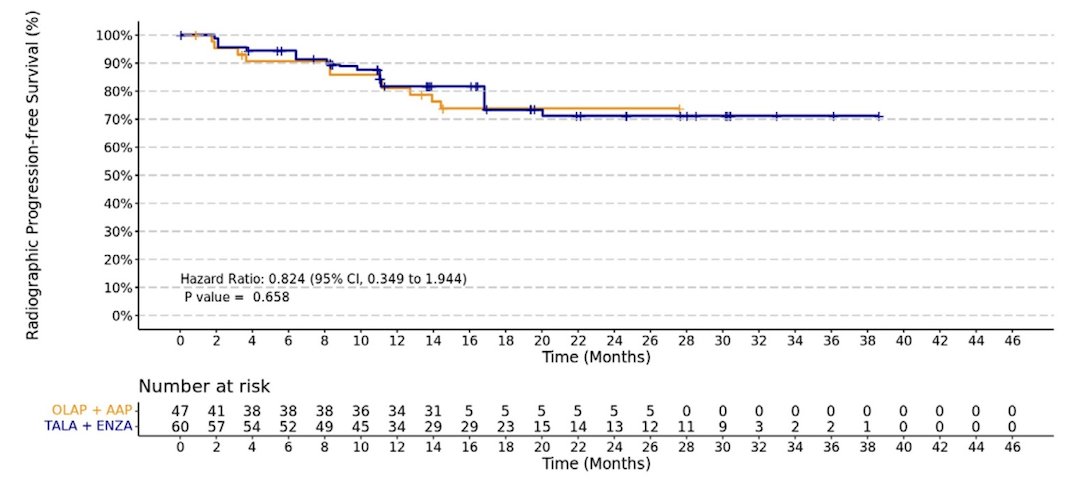

Dr. Thompson acknowledged that this study design is not without limitations. Some of these limitations include the fact that despite adjusting for baseline differences between trials, these MAICs involve comparisons of non-randomized treatment groups, which may be biased by potential unobserved or residual confounding. Additionally, the relative results may also be impacted by differences in the length of study follow-up, including the maturity of the data. Lastly, adjustment for all identified factors was not feasible between PROpel and TALAPRO-2.
Dr. Thompson concluded her presentation with the following key messages:
- These matching-adjusted indirect comparison analyses of TALAPRO-2 and PROpel demonstrate numerically favorable results for TALA+ENZA compared to OLAP+AAP (though not statistically significant).
- This study must be interpreted within its limitations, including the inability to adjust for all characteristics and potential biases due to unobserved trial differences.
Presented by: Allison Thompson, MD, PharmD, Senior Medical Director/Global Clinical Program Lead, Pfizer Inc. New York, New York.
Written by: Julian Chavarriaga, MD – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @chavarriagaj on Twitter during the 2024 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL between May 31st and June 4th.
References:
- Mateo J, de Bono JS, Fizazi K, Saad F, Shore N, Sandhu S, Chi KN, Agarwal N, Olmos D, Thiery-Vuillemin A, Özgüroğlu M, Mehra N, Matsubara N, Young Joung J, Padua C, Korbenfeld E, Kang J, Marshall H, Lai Z, Barnicle A, Poehlein C, Lukashchuk N, Hussain M. Olaparib for the Treatment of Patients With Metastatic Castration-Resistant Prostate Cancer and Alterations in BRCA1 and/or BRCA2 in the PROfound Trial. J Clin Oncol. 2024 Feb 10;42(5):571-583. doi: 10.1200/JCO.23.00339. Epub 2023 Nov 14. PMID: 37963304.
- Agarwal N, Azad AA, Carles J, Fay AP, Matsubara N, Heinrich D, Szczylik C, De Giorgi U, Young Joung J, Fong PCC, Voog E, Jones RJ, Shore ND, Dunshee C, Zschäbitz S, Oldenburg J, Lin X, Healy CG, Di Santo N, Zohren F, Fizazi K. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): a randomised, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303. doi: 10.1016/S0140-6736(23)01055-3. Epub 2023 Jun 4. Erratum in: Lancet. 2023 Jul 22;402(10398):290. PMID: 37285865.
- Saad F, Clarke NW, Oya M, Shore N, Procopio G, Guedes JD, Arslan C, Mehra N, Parnis F, Brown E, Schlürmann F, Joung JY, Sugimoto M, Sartor O, Liu YZ, Poehlein C, Barker L, Del Rosario PM, Armstrong AJ. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108. doi: 10.1016/S1470-2045(23)00382-0. Epub 2023 Sep 12. Erratum in: Lancet Oncol. 2024 May;25(5):e180. PMID: 37714168.