(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 31st and June 4th, 2024 was host to a session addressing techniques to minimize the effects of androgen deprivation therapy (ADT) while explore alternatives in prostate cancer management. Dr. Karen Autio discussed ADT-sparing approaches in both the metastatic castrate sensitive and resistant settings.
Why attempt ADT-sparing approaches? ADT is associated with significant short- and long-term toxicities, summarized below:

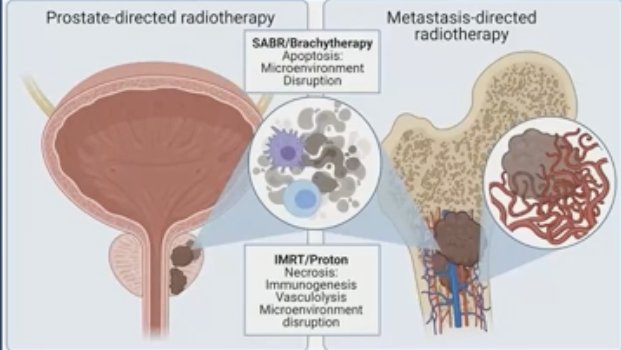
ADT sparing approaches, such as stereotactic ablative radiotherapy (SABR), take advantage of other established therapies and intrinsic drivers of disease.
There are three key randomized trials that have established the role of SABR in oligorecurrent disease: SABR-COMET,1,2 ORIOLE,3 and STOMP.4
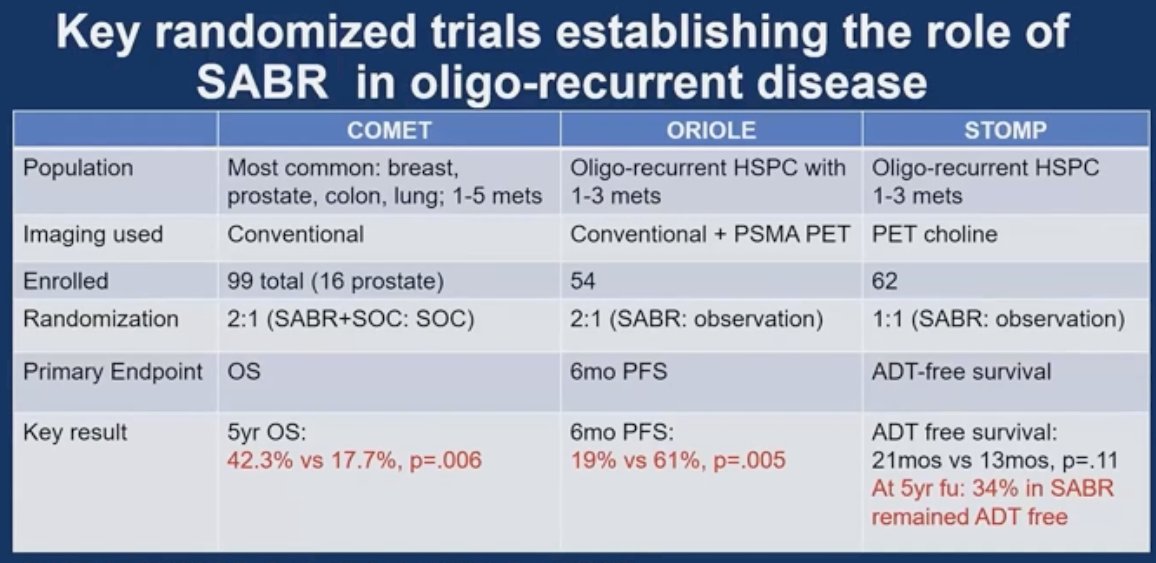
SABR-COMET was a randomized, open-label phase II study of patients with oligometastatic disease (up to five sites) between February 2012 and August 2016. This trial was not restricted to patients with prostate cancer and also included lung, breast, and colorectal cancer patients. Of the 99 patients in this trial, 18 (182%) had prostate cancer. After stratifying by the number of metastases (1–3 versus 4–5), patients were randomized in a 1:2 fashion to receive either palliative standard of care alone or standard of care plus SABR. At a median follow up 51 months, the five-year overall survival rate was 18% in the control arm and 42% in the SABR arm (stratified log-rank p=0.006). The corresponding median overall survivals were 28 months and 50 months, respectively. There was no new grade 2–5 adverse events and no differences in quality of life between the arms.
The ORIOLE trial was a randomized phase II trial of 54 men with metachronous, oligometastatic mHSPC (up to three sites). Metastatic sites were diagnosed via conventional imaging. Between 2016 and 2018, patients were randomized in a 2:1 fashion to receive SABR or observation. The primary outcome was progression at 6 months, defined as serum PSA increase, progression detected by conventional imaging, symptomatic progression, ADT initiation for any reason, or death. Progression at six months occurred in 7 of 36 patients (19%) receiving SABR and 11 of 18 patients (61%) undergoing observation (p=0.005). Treatment with SABR improved median progression-free survival (not reached vs 5.8 months; hazard ratio [HR]: 0.30; 95% CI:0.11–0.81; p=0.002). No toxic effects of grade 3 or greater were observed.
The STOMP trial was a multicenter, randomized phase II trial that prospectively evaluated the effects of metastasis-directed therapy (MDT) for patients with evidence of oligometastatic disease on choline PET/CT (up to three extracranial sites) who had received prior treatment with curative intent and had evidence of biochemical recurrence with testosterone >50 ng/ml (i.e. metachronous, oligometastatic mHSPC). Between 2012 and 2015, 62 patients were randomized 1:1 and MDT was either SABR or metastasectomy. The primary endpoint was time to initiation of ADT (called ADT-free survival). ADT was initiated for symptoms, progression beyond three metastases, or local progression of known metastatic disease. Time to castration resistance was a secondary endpoint (called CRPC-free survival). With a median follow up of 5.3 years, the five-year ADT-free survival was 8% in the surveillance arm compared to 34% for the MDT group (HR: 0.57, 95% CI: 0.38–0.84, log-rank p=0.06). No differences were seen between groups when stratified by nodal versus non-nodal metastases. The secondary endpoint of CRPC-free survival at 5 years was 53% in subjects under surveillance and 76% in those receiving MDT (HR: 0.62, 80% CI: 0.35-1.09).
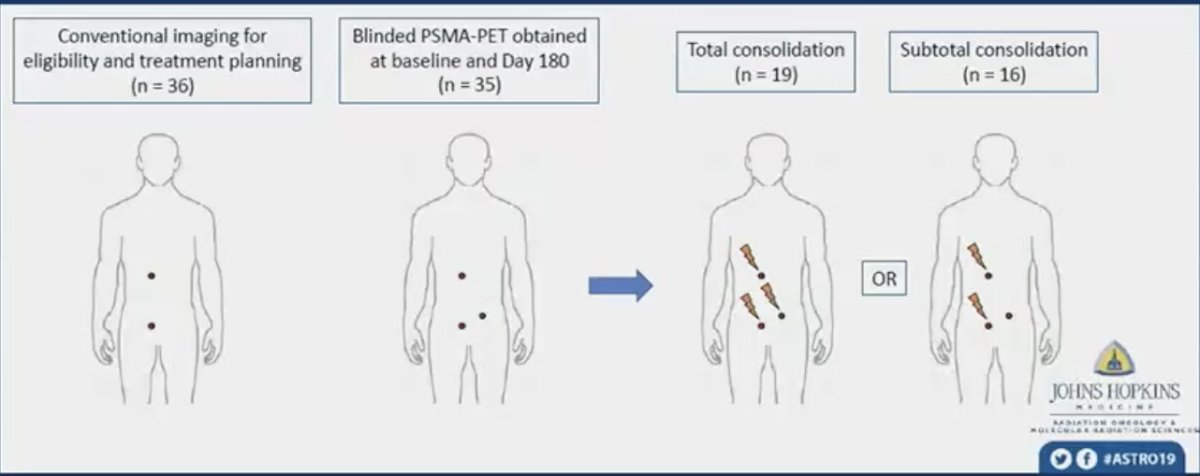
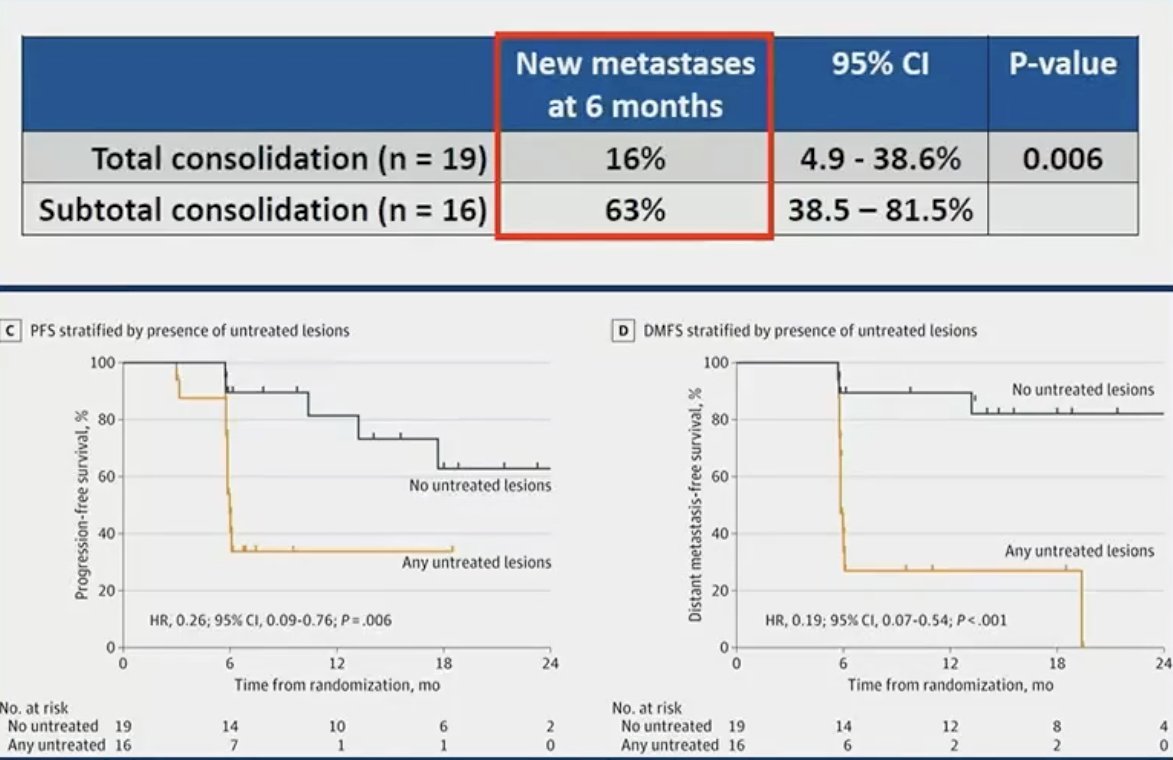
But does PSMA PET/CT (i.e., more sensitive imaging) provide additional information in these patients with evidence of oligometastatic disease on conventional imaging? In the ORIOLE trial, pre-treatment 18F-DCFPyL-PET/CT was performed in all patients assigned to the MDT arm (n = 36). Notably, the treating physicians and patients were blinded to the results of these scans. Of the 36 patients treated with stereotactic ablative radiotherapy, 16 (44.4%) had baseline PET-avid lesions that were not included in the treatment fields. These patients had significantly worse 6-month progression rates of 38% (95% CI: 18.5–61.5%) compared to those with no untreated lesions (5%; 95% CI: 0–26.8%; p = 0.03). Further, those with untreated sites of disease had higher rates of new metastases (per conventional imaging) at 6 months (62.5% versus 15.8%, p=0.006) and worse median distant metastasis-free survival of 6 versus 29 months (HR: 0.19; 95% CI: 0.07–0.54, p<0.001). These results highlight the importance of targeting all sites of disease in the context of MDT for oligometastatic disease, and, particularly, the value of PSMA PET/CT-for defining this with increased sensitivity compared to conventional imaging.
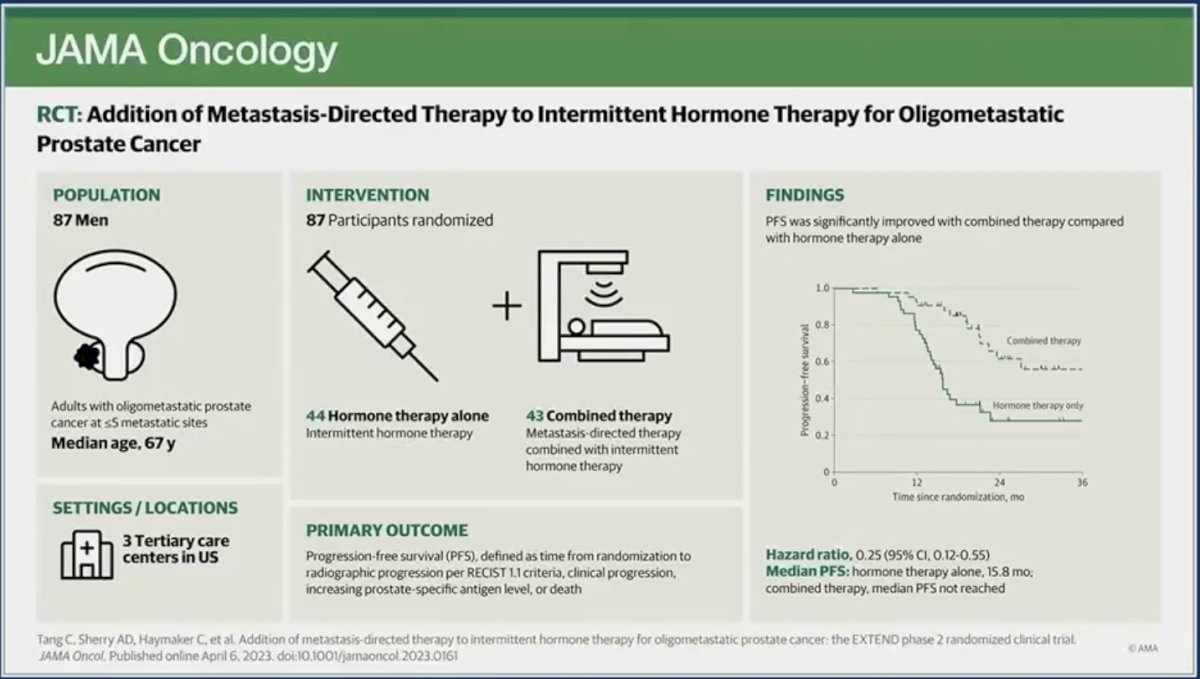
MDT has also been recently evaluated in combination with, not in lieu of, short-term ADT. The EXTEND trial was a single center, phase II randomized trial of 87 oligorecurrent men, mostly with mHSPC (>90%), who were randomized 1:1 to intermittent hormone therapy (ADT +/- androgen receptor pathway inhibitor) +/- MDT (definitive radiation therapy to all sites of disease). All patients had ≤5 metastases, as defined by conventional imaging (75%) or fluciclovine PET/CT (25%). A planned break in hormone therapy occurred 6 months after enrollment, after which hormone therapy was withheld until progression. At a median follow-up of 22 months, progression-free survival was improved in the combined therapy arm (HR: 0.25, 95% CI: 0.12 – 0.55, p<0.001). Significantly, ‘eugonadal’ progression-free survival was also improved with this combination approach (HR: 0.32, p=0.03).5
Based on the current evidence for MDT in this disease space, Dr. Autio noted:
- MDT is supported by phase 2 trials, but no large phase 3 randomized controlled trial data.
- We should counsel patients that MDT is unlikely to cure them.
- When, for how long, and for whom to use ADT/ARPI with MDT remains an open question.
- Other strategies that are ADT sparing in this population are under evaluation:
- Radiopharmaceuticals +/- MDT
- LUNAR: Lu-177-PSMA-617 + SABR versus SABR
- RAVENS: Radium-223 + SABR versus SABR
- BULLSEYE: Lu-177-PSMA-617 versus standard of care
- Radiopharmaceuticals +/- MDT
In contrast to these aforementioned studies which primarily included patients with oligorecurrent (i.e., metachronous disease), Dr. Autio next discussed the role of MDT in patients with de novo metastatic disease. To date, there is no level 1 evidence from randomized controlled trials to support complete avoidance of ADT in this population. The tumor biology of de novo metastatic disease may differ from oligo-recurrent/metachronous disease. Small retrospective series that used multi-modal approaches with fixed courses of ADT have demonstrated variable results. There are multiple ongoing trials using ADT + ARPI + prostate-directed radiation with randomization of the MDT component:
- PLATON: NCT03784755
- TERPS: NCT05223803
- START MET: NCT05209243
- PEACE-6 (OligoPRESTO): NCT04115007
What do the experts say about MDT in this setting? In a consensus poll of the 2022 Advanced Prostate Cancer Consensus Conference (APCCC), the expert attendees were queried regarding the optimal management of patients with low-volume/oligometastatic synchronous mHSPC and 1–3 bone lesions on next-generation imaging:6
- 61% voted for systemic therapy + primary prostate + MDT
- 33% voted for systemic therapy + primary prostate
- 4% voted for MDT + primary prostate and no ADT
- 2% voted for systemic therapy alone
Next moving on to mCRPC, Dr. Autio discussed the rationale for ongoing ADT in castration-resistant prostate cancer. Do we need to continue ADT in these patients? The rationale for this is that some clones remain hormone sensitive and even those with CRPC have some androgen and androgen receptor dependence. Continuation of ADT in CRPC is recommended by the National Comprehensive Cancer Network (NCCN), European Association of Urology (EAU), and American Urological Association (AUA). What is the evidence to support this recommendation?
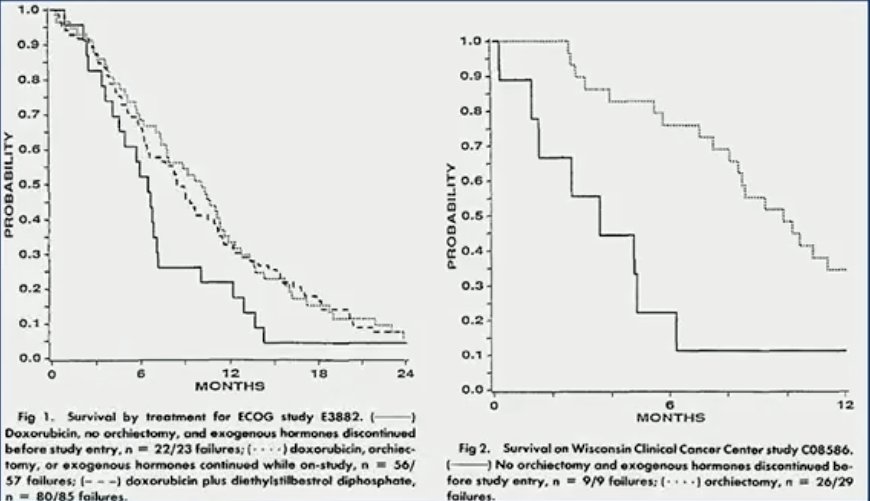
In a 1993 pooled analysis of four clinical trials of secondary therapy for hormone-refractory prostate cancer, Taylor et al. demonstrated that patients who had an orchiectomy performed had a 4–6-month overall survival advantage compared to those who had not had an orchiectomy.7
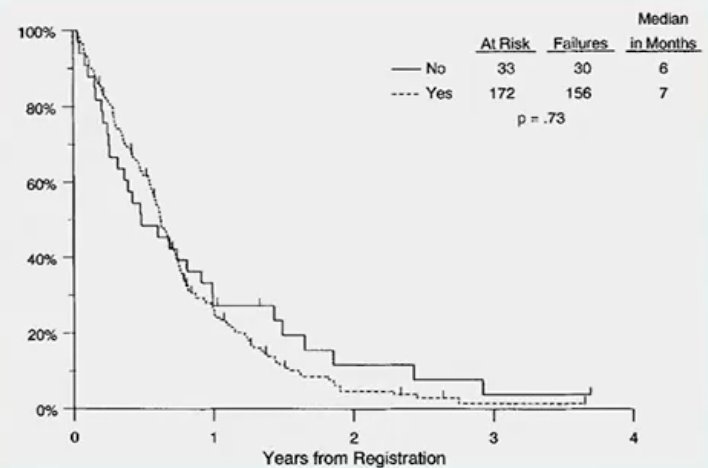
In 1994, Dr. Hussain published the results of a pooled analysis of 205 patients from five consecutive Southwest Oncology Group (SWOG) phase II chemotherapy trials and demonstrated that continued gonadal suppression, via a bilateral orchiectomy, was not associated with improved survival outcomes for castrate-resistant patients.8
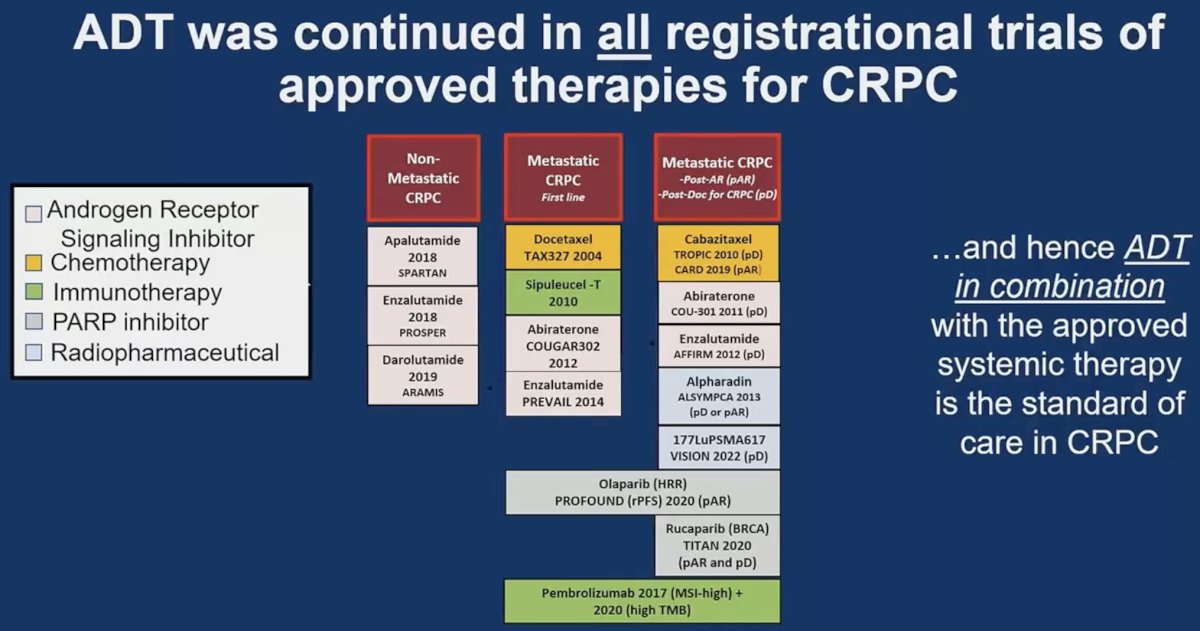
It is important to note that ADT was continued in all registrational trials of approved therapies for CRPC, and hence ADT in combination with the approved systemic therapy is the standard of care in CRPC.
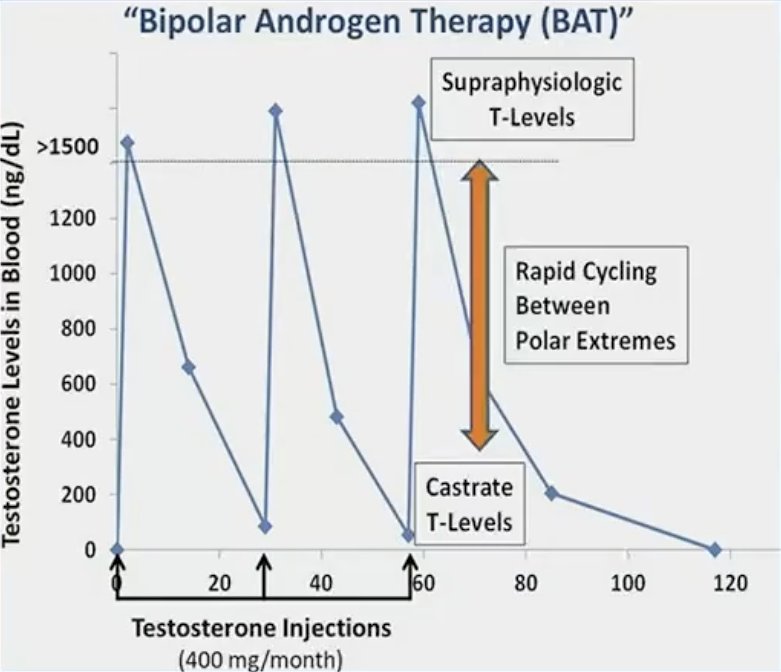
Dr. Autio highlighted bipolar androgen therapy (BAT) as an emerging treatment option for mCRPC patients. BAT involves rapid cycling between high and low testosterone, achieved via ongoing LHRH administration with intramuscular testosterone administration every 28 days. Pre-clinical studies have demonstrated that episodic exposure to supraphysiologic testosterone can downregulate androgen receptor levels that may re-sensitize cells to androgen ablation. Several phase two trials of BAT have demonstrated that this approach can be effective for select patients (TRANSFORMER, RESTORE, COMBAT).
Dr. Autio concluded her presentation as follows:
- In oligorecurrent (metachronous) hormone sensitive metastatic disease detected using molecular imaging, MDT with radiation delays progression-free survival. Deferring ADT can be considered.
- In de novo metastatic disease, there is no randomized trial evidence to support avoidance of ADT. Ongoing trials are assessing a fixed course of ADT in combination with other systemic therapies +/- radiation.
- Continuous ADT remains standard of care in the castration-resistant setting. The most mature data challenging this paradigm is bipolar androgen therapy.
Presented By: Karen A. Autio, MD, MSc, Assistant Attending Physician, Genitourinary Oncologist & Early Drug Development Specialist, Memorial Sloan Kettering Cancer Center, New York, NY
Written By: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, May 31 – Tues, June 4, 2024
References:
- Palma DA, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): a randomised, phase 2, open-label trial. Lancet. 2019;393(10185):2051-2058.
- Palma DA, Olson R, Harrow S, et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J Clin Oncol. 2020;38(25):2830-2838.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate CancerThe ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020;6(5):650-659.
- Ost P, Reynders D, Decaestecker K, et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018;36(5):446-453.
- Tang C, Sherry AD, Haymaker C, et al. Addition of Metastasis-Directed Therapy to Intermittent Hormone Therapy for Oligometastatic Prostate Cancer: The EXTEND Phase 2 Randomized Clinical Trial. JAMA Oncol. 2023;9(6): 825-834.
- Gillessen S, Bossi A, Davis ID, et al. Management of patients with advanced prostate cancer-metastatic and/or castration-resistant prostate cancer: Report of the Advanced Prostate Cancer Consensus Conference (APCCC) 2022. Eur J Cancer. 2023;185: 178-215.
- Taylor CD, Elson P, Trump DL. Importance of continued testicular suppression in hormone-refractory prostate cancer. J Clin Oncol. 1993;11(11): 2167-72.
- Hussain M, Wolf M, Marshall E, Crawford ED, Eisenberger M. Effects of continued androgen-deprivation therapy and other prognostic factors on response and survival in phase II chemotherapy trials for hormone-refractory prostate cancer: a Southwest Oncology Group report. J Clin Oncol. 1994;12(9): 1868-75.