(UroToday.com) The 2022 GU ASCO Annual meeting included a renal cell carcinoma (RCC) trials in progress session featuring PIVOT IO 011, presented by Dr. Martin Voss, a phase 1/2 study evaluating of bempegaldesleukin plus nivolumab and TKI versus nivolumab and TKI alone in patients with previously untreated advanced or metastatic RCC.
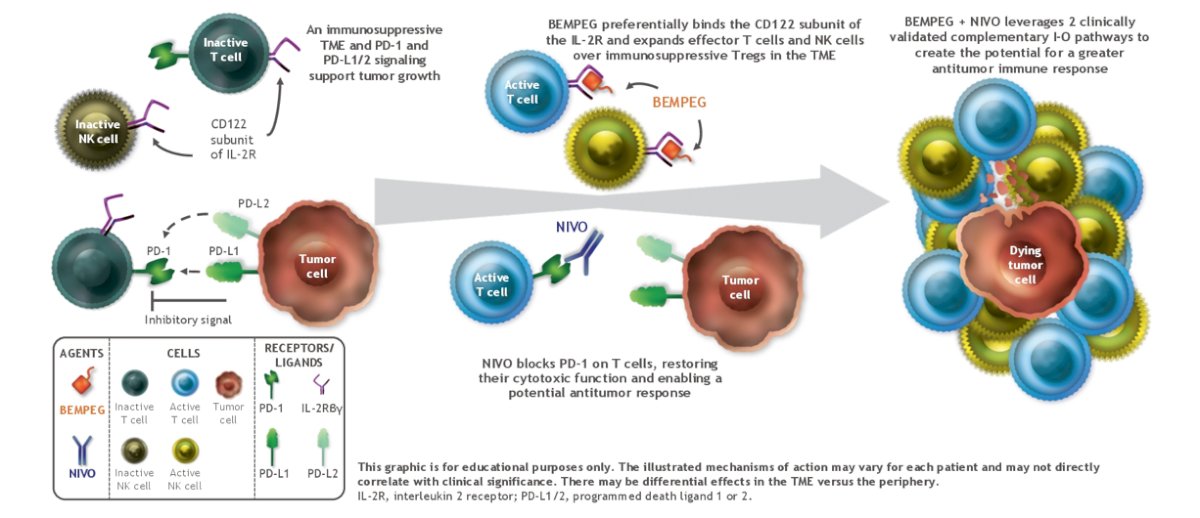
The current standard of care for advanced RCC utilizes immune checkpoint inhibitors (ICIs) and targeted agents. Novel combinations of these agents, such as nivolumab + TKIs, have demonstrated clinical benefit over TKI monotherapy. In CheckMate 9ER, nivolumab + cabozantinib in advanced RCC demonstrated clinically meaningful efficacy results and a favorable safety profile [1], and was FDA approved (January 2021). High-dose interleukin-2 (IL-2) was used historically for durable responses in metastatic RCC but had unfavorable toxicity with complex inpatient treatment regimens. Bempegaldesleukin, an immunostimulatory IL-2 cytokine prodrug, is engineered to deliver a controlled, sustained, and preferential signal to the clinically validated IL-2 pathway. Preferential binding of bempegaldesleukin to the IL-2 heterodimeric receptor (IL-2Rβγ) activates and expands CD8+ T cells and NK cells over immunosuppressive Tregs. Bempegaldesleukin + nivolumab leverages two complementary pathways that demonstrate antitumor activity:
In the phase 1/2 PIVOT-02 study, bempegaldesleukin + nivolumab displayed encouraging antitumor activity in patients with metastatic RCC, with a tolerable safety profile. The clinical activity and the manageable, non-overlapping toxicity profiles of the individual agents in this combination warrants exploration of triplet regimens in previously untreated advanced RCC.
PIVOT IO 011 (NCT04540705) is a 2-part, phase 1/2, randomized, open-label study assessing the safety and efficacy of bempegaldesleukin + nivolumab + TKI triplet in patients with untreated advanced RCC or metastatic RCC. In Part 1, patients will receive bempegaldesleukin + nivolumab + TKI (Part 1A: axitinib or Part 1B: cabozantinib; n≈6–24 patients in each TKI arm). While bempegaldesleukin + nivolumab dosing will remain consistent across phases, each TKI will have two doses evaluated in Part 1, and results will determine the recommended phase 2 dose for axitinib/cabozantinib in Part 2. In Part 2, patients will be randomized 1:1 to receive either bempegaldesleukin + nivolumab + cabozantinib or nivolumab + cabozantinib (N≈250), stratified by IMDC prognostic score and prior nephrectomy status. If the cabozantinib triplet has an unacceptable toxicity profile, Part 2 may be amended to use the axitinib triplet. The PIVOT IO 011 study design is as follows:
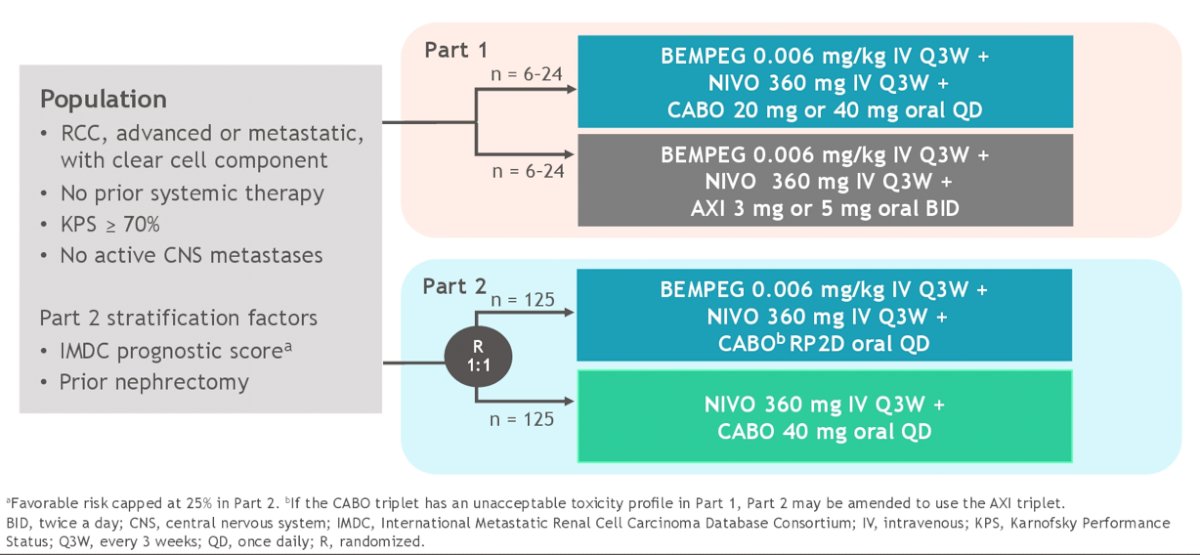
Key inclusion criteria include:
- Advanced RCC or metastatic RCC with clear cell component
- No prior systemic therapy for RCC, except 1 prior adjuvant/neoadjuvant therapy for completely resectable RCC (must have included an anti–VEGF agent with recurrence ≥6 months after last dose)
- Karnofsky PS ≥70%
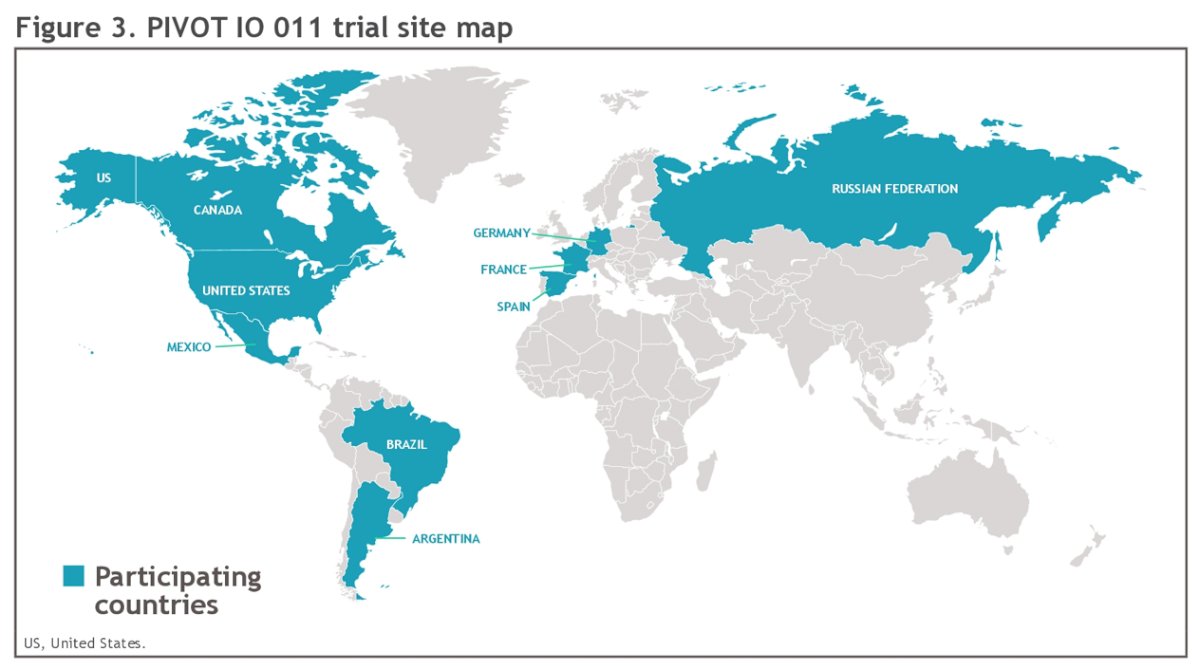
Key exclusion criteria include (i) active CNS brain/leptomeningeal metastases, (ii) active, known, or suspected autoimmune disease, and (iii) inadequately treated adrenal insufficiency. The primary endpoints in Part 1 are dose-limiting toxicities and safety, and in Part 2 are overall response rate per RECIST v1.1 by investigator. Secondary endpoints in Part 2 include progression-free survival, overall survival, safety. Duration of bempegaldesleukin + nivolumab will be ≤2 years, and treatment with TKI will continue until disease progression. This study is currently recruiting eligible patients at six 6 sites in 2 countries, and enrollment in part 2 will be expanded to additional sites across 9 countries:
Presented By: Martin H Voss, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Co-Authors: Scott S. Tykodi, Marc-Oliver Grimm, Hans J. Hammers, Brian I. Rini, Nizar M. Tannir, Anila H. Qureshi, Vicky Tsipouri, Moana Hodari, Shruthi Ravimohan, Melissa Andrea Reimers
Affiliations: The University of Washington and Fred Hutchinson Cancer Research Center, Seattle, WA, Universitätsklinikum Jena, UT Southwestern Medical Center, Dallas, TX, Vanderbilt-Ingram Cancer Center, Nashville, TN, UT MD Anderson Cancer Center, Houston, TX, Bristol Myers Squibb, Princeton, NJ, Washington University in St. Louis, St. Louis, MO
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, Thursday Feb 17 – Saturday Feb 19, 2022
References: