(UroToday.com) On the second day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2023 focussing on urothelial cancer, the Trials in Progress Poster Session B included a presentation from Dr. Neal Shore on cohort C of the phase II KEYNOTE-057 trial assessing pembrolizumab with vibostolimab or favezelimab for patients with high-risk (HR) bacillus Calmette-Guérin (BCG)-unresponsive non–muscle-invasive bladder cancer (NMIBC).
There is a considerable unmet clinical need for patients with high-risk (HR) bacillus Calmette-Guérin (BCG)-unresponsive non–muscle-invasive bladder cancer (NMIBC). In cohort A of the phase 2 KEYNOTE-057 study (NCT02625961), the PD-1 inhibitor pembrolizumab showed promising antitumor activity, with 41% of patients with HR BCG-unresponsive carcinoma in situ (CIS) of the bladder ± papillary tumors achieving a CR at 3 months with a median DOR of 16.2 months. Based on these results, pembrolizumab was approved in the United States for treatment of patients with BCG-unresponsive HR NMIBC with CIS ± papillary tumors who are ineligible for or have elected not to undergo radical cystectomy (RC). However, novel combinations that improve the efficacy of pembrolizumab are needed. One such treatment paradigm is combination therapy. Immune checkpoints TIGIT and LAG-3 have been shown to contribute to treatment resistance in many cancers, and their inhibition may enhance the activity of pembrolizumab. Thus, cohort C of KEYNOTE-057 will evaluate the efficacy and safety of coformulations of pembrolizumab and TIGIT inhibitor vibostolimab or LAG-3 inhibitor favezelimab in patients with HR BCG-unresponsive NMIBC with CIS ± papillary tumors.
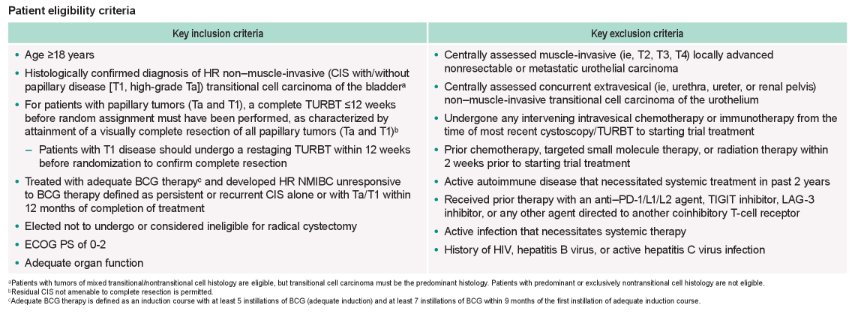
Cohort C of this trial will enroll adult patients with histologically confirmed HR NMIBC that is unresponsive to BCG (defined as persistent or recurrent CIS alone or with Ta/T1 ≤12 months of completion of adequate BCG therapy) who are ineligible for or elect not to undergo RC, have CIS ± papillary tumors at baseline (CIS alone, Ta + CIS or T1 + CIS), and have an ECOG score of 0-2 (NCT02625961).
The authors aim to accrue approximately 60 patients who will be randomly assigned in a 1:1 fashion to Arm 1 (coformulation of pembrolizumab 200 mg and vibostolimab 200 mg) or Arm 2 (coformulation of pembrolizumab 200 mg and favezelimab 800 mg) IV Q3W (≤35 administrations) until central pathology-confirmed ≥T1 at any time point or persistent or recurrent CIS or high-grade ≥Ta at the 24-week efficacy review or thereafter. Patients with central pathology–confirmed low-grade pTa at any time point may continue treatment following resection of visible tumors. In the absence of disease persistence/recurrence or progression, treatment will continue until unacceptable toxicity, decision to withdraw, or administrative reasons.

Patients will undergo tumor evaluations every 12 weeks until year 2, then every 24 weeks thereafter for up to 5 years to assess the primary efficacy end point of 12-month CR rate of HR NMIBC as determined by cystoscopy, cytology, biopsy, and radiologic imaging by central pathology and radiology review. There are a number of additional secondary efficacy end points including DOR of HR NMIBC in responders; overall CR rate and CR rate at 3 and 6 months; PFS to worsening of grade, stage, or death; PFS to muscle-invasive or metastatic disease or death; and OS. Efficacy will be evaluated in all patients who received at least 1 dose of study treatment and have a baseline evaluation consisting of pre-enrollment cystoscopy, TURBT/biopsy, urine cytology, and baseline CT urography imaging. Additionally, the authors will seek to characterize the safety and tolerability in all patients who received at least 1 dose of study treatment.
Presented by: Neal D. Shore, MD, FACS, Medical Director, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC