(UroToday.com) The 2023 GU ASCO annual meeting included a trials in progress session for renal cell carcinoma, featuring a presentation by Dr. Elshad Hasanov discussing the trial design of a phase 1b/2 study of combination 177Lu girentuximab plus cabozantinib and nivolumab in treatment naïve patients with advanced clear cell RCC.
Indeed, complete response is still a rare event in patients with advanced clear cell RCC. The combination of nivolumab plus cabozantinib was recently approved for the first-line treatment of clear cell RCC based on the CheckMate 9ER phase 3 study demonstrating improved progression-free survival (PFS) and objective response rate (ORR) in comparison to sunitinib.1 However, the complete response rate was only 9%. Since the anti-tumor effects of immune checkpoint inhibitors are dependent on the presence of activated tumor-infiltrating T cells, drugs that could synergize with T cells’ anti-tumor activity can allow us to improve complete response rates. Activation of the cGAS-STING pathway which is induced by radiation-induced DNA damage, is one promising mechanism that has been investigated. Many studies have shown that radiation treatment augments immune checkpoint inhibition. However, it is not always possible to radiate all metastatic lesions. Therefore, targeted peptide receptor radionuclide therapies, have been developed by conjugating radioisotopes to receptor binding analogs targeting specific cancer cell surface proteins, thereby delivering targeted radiation to cancer cells in the body with minimal damage to surrounding healthy cells. 177Lu girentuximab is the first antibody-radioisotope designed for clear cell RCC, targeting carbonic anhydrase 9-expressing cells, which includes >90% of clear cell RCC. It has been tested in metastatic clear cell RCC as a single agent and shown to be safe and effective in stabilizing disease in 57% of patients:
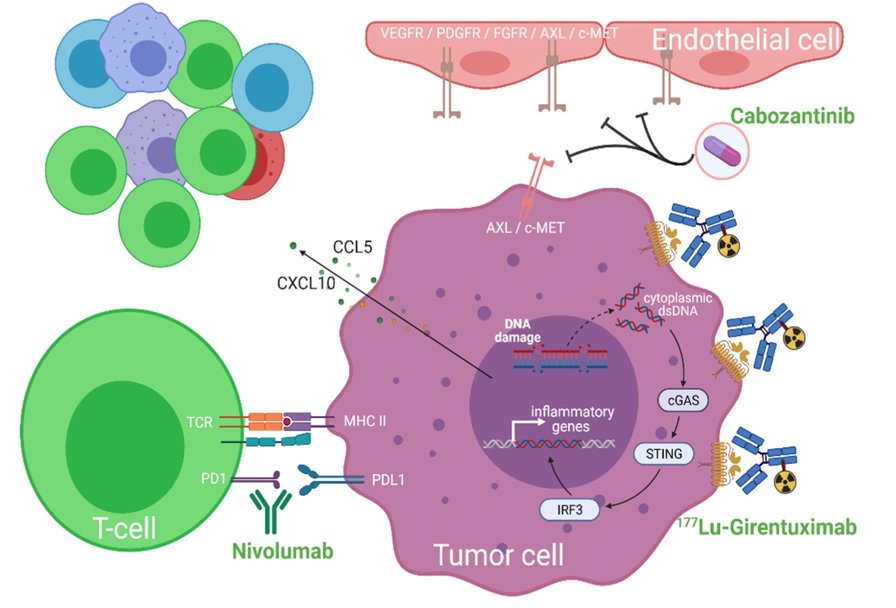
In this study, Dr. Hasanov and colleagues hypothesize that 177Lu girentuximab-induced DNA damage will potentiate the STING pathway, and this activation will synergize with nivolumab and cabozantinib to promote trafficking and infiltration of activated T cells to tumors and achieve higher complete response rates.
Up to 100 patients with treatment naïve, biopsy-proven clear cell RCC with adequate organ/marrow function with ≥1 evaluable lesion by RECIST 1.1 will be enrolled. A 5-patient safety lead-in will evaluate myelosuppression. Ongoing safety, and futility monitoring will employ a Bayesian approach. The sample size was chosen for reasonable operating characteristics to distinguish a complete response rate (primary endpoint) of 18% as better than 9% using a beta (0.09, 0.91) prior. Secondary endpoints are ORR, PFS by RECIST 1.1, and overall survival. 177Lu-girentuximab 1480 MBq/m2 (61% of single agent maximum tolerated dose) will be administered every 12 weeks for up to 3 cycles. Starting with the second cycle, nivolumab and cabozantinib will be added at standard dose. The trial design is as follows:

To explore the effects of the treatment on inducing activated T cell infiltration, patients will undergo pre/post-treatment PET scan with [18F]F-AraG radiotracer, as well as biopsies for single cell, spatial transcriptomics and proteomics studies.
Presented by: Elshad Hasanov, MD, PhD, University of Texas MD Anderson Cancer Center, Houston, TX
Co-Authors: Lesley Flynt, Rebecca Slack Tidwell, Hyunsoo Hwang, Roserika Brooks, Lauren Michelle King, Travis Solley, Dahlia Mack, Yuko Yamamura, Colin Hayward, Aradhana M. Venkatesan, Eric Jonasch
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, Thurs, Feb 16 – Sat, Feb 18, 2023.
References: