(UroToday.com) The 2023 GU ASCO annual meeting included a session on prostate cancer, featuring a presentation by Dr. Atsunori Yorozu discussing results from TRIP/TRIGU0907, a multicenter, randomized, phase 3 trial of trimodality therapy with I-125 brachytherapy, external beam radiation therapy, and long- versus short-term ADT for localized high-risk prostate cancer. According to the ASCO/Cancer Care Ontario Joint Guideline Update 2017, for patients with high-risk prostate cancer receiving EBRT and ADT, brachytherapy boost should be offered to eligible patients. The TRIP trial was designed to determine whether 30 months of ADT was superior to 6 months of ADT when combined with brachytherapy and external beam radiotherapy for localized high-risk prostate cancer.
This trial was completed in 37 hospitals in Japan. Men between 40 to 79 years old with stage T2c-3a prostate cancer, or a PSA >20 ng/ml or a Gleason score >7 received 6 months of ADT combined with I-125 brachytherapy at a dose of 110 Gy, followed by external beam radiotherapy of 45 Gy. Patients were randomly assigned either no further treatment (short arm) or 24 months of adjuvant ADT (long arm) after stratification. The trial design for TRIP is as follows:
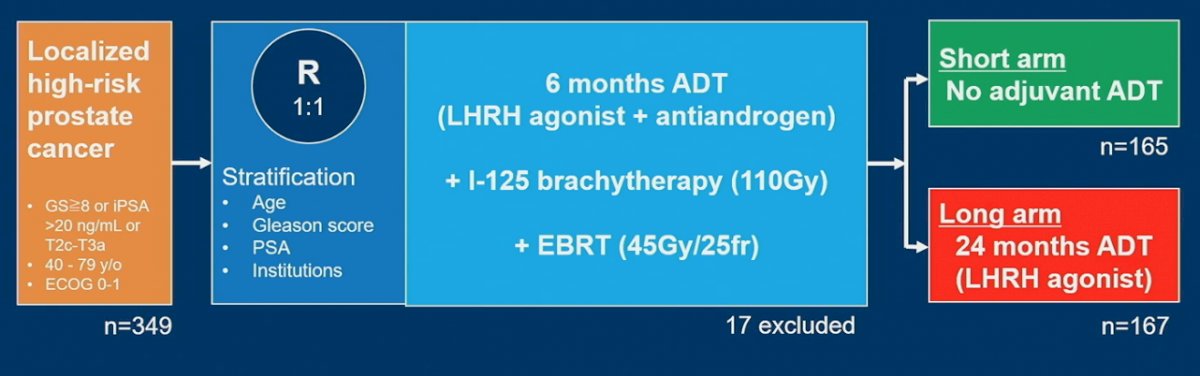
The primary endpoint was biochemical progression-free survival using the Phoenix definition of failure. Secondary endpoints included:
- Clinical progression
- Metastasis
- Salvage treatment
- Disease-specific survival
- Overall survival
- Grade 3 or higher of adverse events
An intention-to-treat analysis was conducted with survival estimates determined using competing risk analyses.
Of 332 patients, 165 were randomized to the short and 167 to the long arm of adjuvant ADT. The two arms were well balanced with a median age of 70 years (range 50-79), initial median PSA of 16.2 ng/mL (range 3-182), 32% Gleason 8, 19% Gleason 9-10, and 43% with multiple high-risk features. The median follow-up periods were 9.43 and 9.24 years, respectively, over which 24 patients died in each arm. The cumulative incidence for biochemical progression in the short vs. long arm were 10.4% (95% CI 6.62-16.42%) vs 9.5% (95% CI 5.85-15.46%) at 9 years, respectively (p=0.65):

The cumulative incidences for clinical progression, distant metastases, salvage treatment, and disease-specific mortality events were not significantly different between the two arms. The overall survival rates of the short arm vs long arm were 87.2% (95% CI 82.13-92.63%) and 85.9% (95% CI 80.41-91.77%) at 9 years, respectively (p=0.91). Endocrine-related grade 3 morbidity for short arm vs long arm was 0.6% vs 1.8% (p=0.62), and radiation-related grade 3 morbidity was 1.2% vs 0.6% (p=0.62).
Dr. Yorozu concluded this presentation discussing results from TRIP/TRIGU0907 with the following concluding messages:
- This trial failed to show a benefit of long-term vs short-term ADT with regards to biochemical PFS in selected high-risk prostate cancer patients treated in conjunction with combined radiation therapy
Clinical trial information: UMIN000003992
Presented by: Atsunori Yorozu, MD, PhD, National Hospital Organization Tokyo Medical Center, Tokyo, Japan
Co-Authors: Mikio Namiki, Shiro Saito, Shin Egawa, Hiroshi Yaegashi, Konaka Hiroyuki, Tetsuo Momma, Takashi Fukagai, Nobumichi Tanaka, Toshio Ohashi, Hiroyuki Takahashi, Atsushi Mizokami, Yoko Nakagawa, Takashi Kikuchi, Nelson Stone
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, Thurs, Feb 16 – Sat, Feb 18, 2023.