(UroToday.com) The 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between January 25th and 27th was host to a urothelial carcinoma trials in progress poster session. Dr. Neal Shore presented the study design and provided an update for the phase 3 KEYNOTE-676 Cohort A trial of BCG +/- pembrolizumab for patients with high-risk non-muscle invasive bladder cancer (HR NMIBC) that persists/recurs following BCG induction.
Intravesical instillation of bacillus Calmette-Guérin (BCG) is standard of care for patients with HR NMIBC. However, many patients have persistent/recurrent HR NMIBC after BCG induction and are at a particularly increased risk for disease progression.
PD-L1 expression is correlated with bladder cancer severity and outcomes; PD-L1 expression in the tumor microenvironment can attenuate responses to BCG by repressing activated T cells. PD-1 is an immune checkpoint receptor known to play a role in tumor immune evasion. Pembrolizumab is a humanized monoclonal antibody that binds to PD-1, preventing interaction with its ligands, PD-L1 and PD-L2. In the phase 2 KEYNOTE-057 trial, pembrolizumab monotherapy demonstrated efficacy in patients with BCG-unresponsive HR NMIBC and carcinoma in situ (CIS), with a safety profile consistent with that of other studies, with a centrally assessed complete response (CR) rate at 3 months of 41%.1
The combination of pembrolizumab and BCG has been shown to be safe and may increase the antitumor activity of BCG. KEYNOTE-676 (NCT03711032) is an open-label, comparator-controlled, phase 3 study designed to compare pembrolizumab + BCG with BCG monotherapy in patients with HR NMIBC. Dr. Shore and colleagues presented the study design of cohort A, which will enroll patients with persistent or recurrent HR NMIBC following BCG induction therapy.
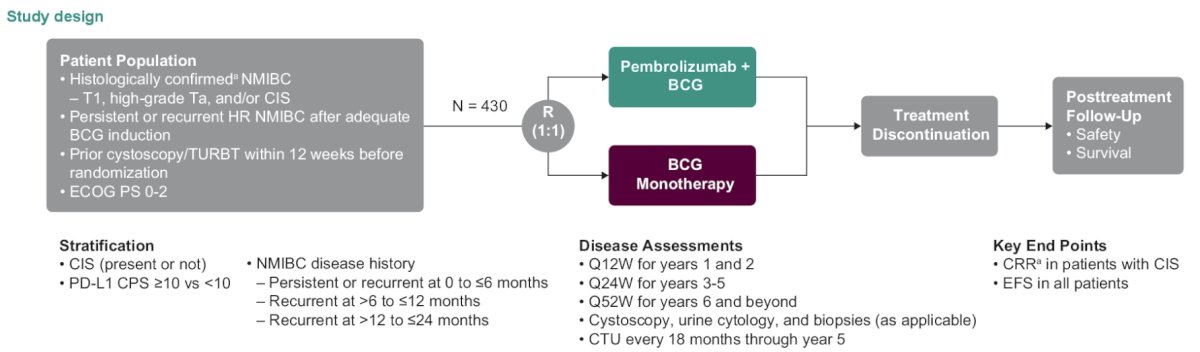
Approximately 430 patients with histologically confirmed HR NMIBC will be enrolled, and patients will be randomly assigned 1:1 to receive pembrolizumab + BCG or BCG monotherapy. Pembrolizumab will be administered intravenously at the standard dose of 200 mg every 3 weeks, whereas BCG (50 mg) will be administered via intravesical instillation, first as induction therapy (once a week for 6 weeks) and then as maintenance therapy, with 12-week intervals (3 and 6 months) for the first and second maintenance cycles and then at 6-month intervals. Treatment with pembrolizumab will continue until 35 doses have been administered (approximately 2 years), and treatment with BCG will continue for a total of 145 weeks (approximately 3 years).
Treatment in either arm will be discontinued if the patient has:
- Persistent/recurrent high-risk disease
- Progressive disease
- Unacceptable toxicity
- Intercurrent illness preventing further administration
- After investigator or patient decision to withdraw
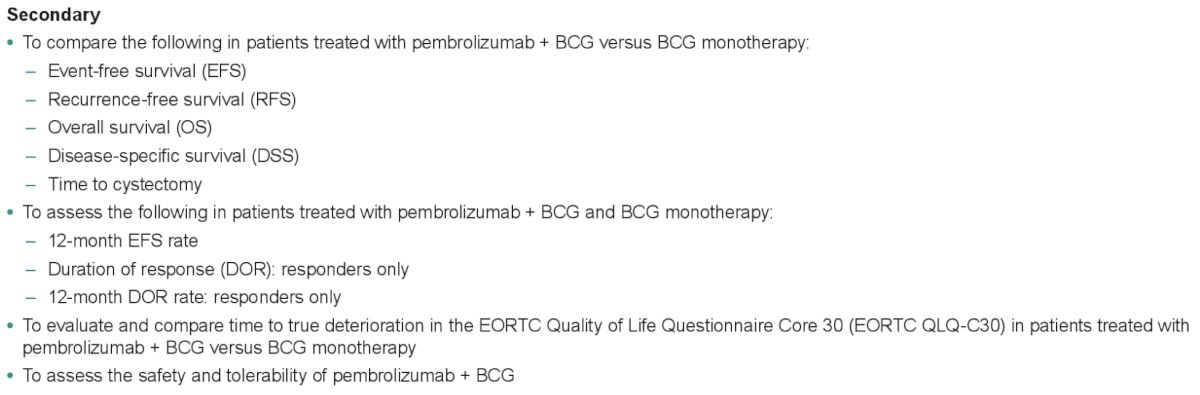
The primary study objective is to compare CR rates between the two arms in CIS patients. CR will be defined as the absence of HR NMIBC, confirmed by cystoscopy, urine cytology, radiologic assessments, and biopsy (as applicable). The other study outcomes/objectives are summarized below:
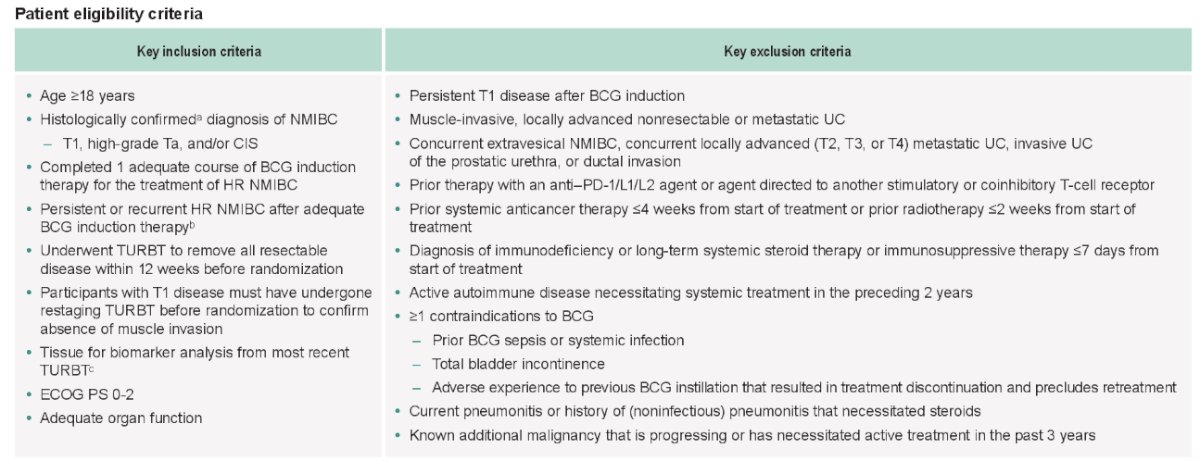
The full study eligibility criteria are summarized below:
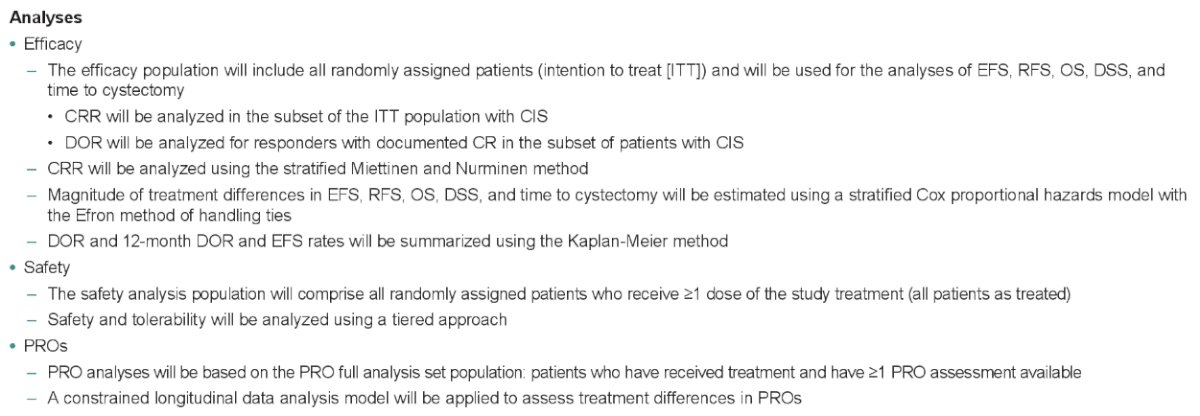
Planned statistical analyses are summarized below:
The KEYNOTE-676 trial is enrolling patients in Cohort A at sites in Asia, Australia, Europe, and North America.
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, San Francisco, CA, January 25th – January 27th, 2024
Related content: Combining Pembrolizumab and BCG Immunotherapies: The KEYNOTE-676 Trial in High-Risk NMIBC - Neal Shore
References:
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.