(UroToday.com) The 2021 American Society for Radiation Oncology (ASTRO) Hybrid Annual Meeting’s included a session on biomarkers and salvage radiotherapy and discussion by Dr. Alan Dal Pra regarding the performance of a genomic classifier within a phase 3 randomized trial of dose escalated salvage radiotherapy after radical prostatectomy.
Genomic classifiers can independently prognosticate prostate cancer outcomes and may help individualize treatment intervention. Pre-salvage PSA is an important prognostic and a predictive factor for salvage radiotherapy and androgen deprivation therapy post-prostatectomy. In the study presented at ASTRO 2021, Dr. Dal Pra and colleagues assessed the role of the genomic classifier in patients treated within a contemporary phase 3 trial.
The SAKK 09/10 trial (NCT01272050) is a multicenter, randomized phase 3 trial performed in 24 centers in Switzerland, Germany, and Belgium. Patients with biochemical progression (PSA >0.1 to 2 ng/mL at randomization) were randomized to 64 Gy versus 70 Gy to the prostate bed; no ADT or pelvic nodal radiotherapy was used. The results of this study were recently published in European Urology [1] and there was no difference in failure from biochemical progression between the two groups after six years of follow-up:

There was a pre-specified statistical plan (prior to the trial primary endpoint analysis) to assess the impact of the genomic classifier on clinical outcomes. Radical prostatectomy samples were centrally reviewed for the highest-grade tumor, and after passing quality control, samples were run on the Decipher assay. Additionally, the study followed the PRoBE and REMARK criteria. The primary endpoint for the study was time to freedom from biochemical progression, secondary endpoints included clinical progression free survival and receipt of ADT, and exploratory endpoints included rapid biochemical progression (<= 18 months), distant metastases, and metastasis-free survival. In this exploratory sub-analysis, the primary endpoint was failure from biochemical progression to PSA at randomization (<= 0.5 (early salvage radiotherapy) versus >0.5 (late salvage radiotherapy), a trial stratification variable). Cox multivariable analysis adjusting for age, T-category, Gleason score, persistent PSA after radical prostatectomy, and randomization arm were performed.
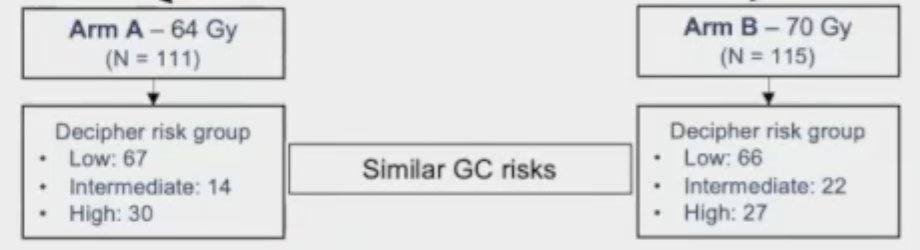
Among contemporary samples, there was a high lab quality control passing rate of >97%, which included 226 unique patients that subsequently underwent a Decipher test (n = 111 in Arm A – 64 Gy; n = 115 in Arm B – 70 Gy). Overall, genomic classifier risks were comparable between the two arms.
In this study, cohort characteristics were representative of the full SAKK 09/10 cohort, with comparable stratification variables in Arm A and Arm B. For genomic classifier high versus low/intermediate, the hazard ratios are as follows:
- Biochemical progression: HR 2.22 (95% CI 1.37-3.58)
- Clinical progression: HR 2.29 (95% CI 1.32-3.98)
- Salvage ADT: HR 2.99 (95% CI 1.50-5.95)
For genomic classifier high- versus low/intermediate disease in the salvage radiotherapy subgroup, hazard ratios were:
- For early salvage radiotherapy (PSA <= 0.5 ng/mL): HR 1.84 (95% CI 0.99-3.43)
- For late salvage radiotherapy (PSA > 0.5 ng/mL): HR 3.07 (95% CI 1.39-6.80)
Additionally, the prognostic performance of Decipher score within pre-salvage radiotherapy PSA subgroups showed that for freedom from biochemical progression for a PSA at randomization > 0.5 ng/mL had a hazard ratio of 1.23 (95% CI 1.07-1.41).
Dr. Dal Pra highlighted several important discussion points from this trial:
- In a phase 3 randomized trial with a prespecified hypothesis, the genomic classifier adds independent prognostic performance
- The use of a genomic classifier can complement pre-salvage radiotherapy PSA and provide further risk stratification
- The results suggest that for patients with a genomic classifier high score, intervening when the PSA burden is lowest results in improved outcomes
- Pre-salvage radiotherapy PSA subgroup analysis remains exploratory and hypothesis-generating
- A low number of events and short follow-up (6 years) precluded distant metastasis and OS analysis
- In line with NRG/RTOG 9601 data suggesting that patients with higher pre-salvage radiotherapy and higher genomic classifier score derive the most benefit from hormonal therapy
Dr. Dal Pra concluded his presentation with the following take-home messages:
- Independent of standard clinicopathologic variables and radiotherapy dose, patients with a high-genomic classifier score were more than twice as likely than patients with low/intermediate-genomic classifier to experience biochemical progression, clinical progression, and receive salvage ADT
- High-genomic classifier patients who received late salvage radiotherapy (PSA > 0.5 ng/mL) had nearly 90% risk of recurrence by 5 years post-salvage radiotherapy
- This study represents the first contemporary RCT in patients treated with salvage radiotherapy alone that has validated the prognostic utility of a genomic classifier. It provides level 1 evidence for the use of the genomic classifier for personalizing postoperative salvage radiotherapy
Presented by: Alan Dal Pra, MD, Department of Radiation Oncology, University of Miami, Miami, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 American Society for Radiation Oncology (ASTRO) Hybrid Annual Meeting, Sat, Oct 23 – Wed, Oct 27, 2021.
References:
- Ghadar P, Hayoz S, Bernhard J, et al. Dose-intensified versus conventional-dose salvage radiotherapy for biochemically recurrent prostate cancer after prostatectomy: The SAKK 09/10 Randomized Phase 3 Trial. Eur Urol. 2021;80(3):306-315.