(UroToday.com) The 2023 American Society for Radiation Oncology (ASTRO) 65th Annual Meeting held in San Diego, CA between October 1st and 4th, 2023 was host to a session on stereotactic radiotherapy for renal cell cancer. Dr. Shankar Siva discussed technical considerations, response assessment, and challenging cases in primary renal stereotactic ablative radiotherapy (SABRT).
One of the main technical challenges for renal SABR is respiratory induced-kidney motion. In an analysis of 71 consecutive patients with ‘normal’ kidneys who had a 4-dimensional CT performed, Siva et al. previously demonstrated that the mean displacement was 0.74-0.75 cm on both sides. However, there were some extreme outliers, with maximum amplitudes of 2.3 to 3.3 cm.1 This is consistent with overall data from the literature with a systematic review in 2014 demonstrating that the majority of individuals having mean renal motion of <10 mm. As such, Dr. Siva recommended to include the full inhale and exhale phases while contouring. If using an internal target volume (ITV) concept, one should not rely on maximum intensity projection (MIP) averages and should carefully go through respiratory bins and understand any artefacts.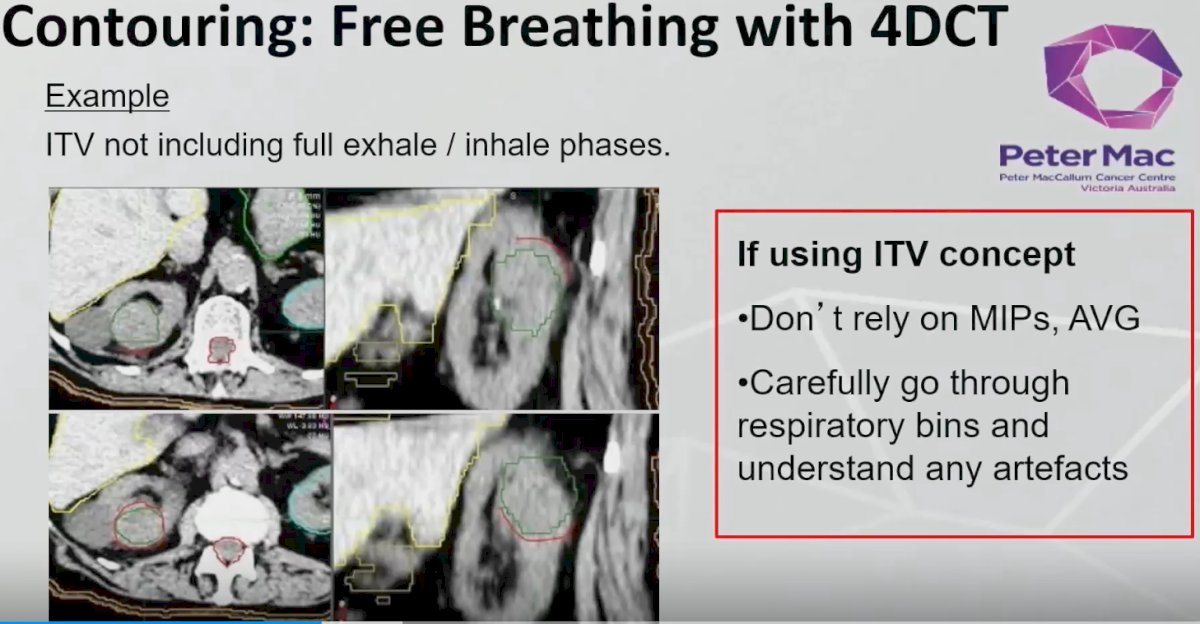
Drawing on his own institutional practices, Dr. Siva noted that since 2012 at The Peter MacCallum Cancer Centre, lesions 4 cm in size or smaller are treated with single session SABR (26 Gy in 1 fraction). For lesions >4 cm, patients receive 3 sessions of SABR at 42 Gy in 3 fractions, administered twice weekly.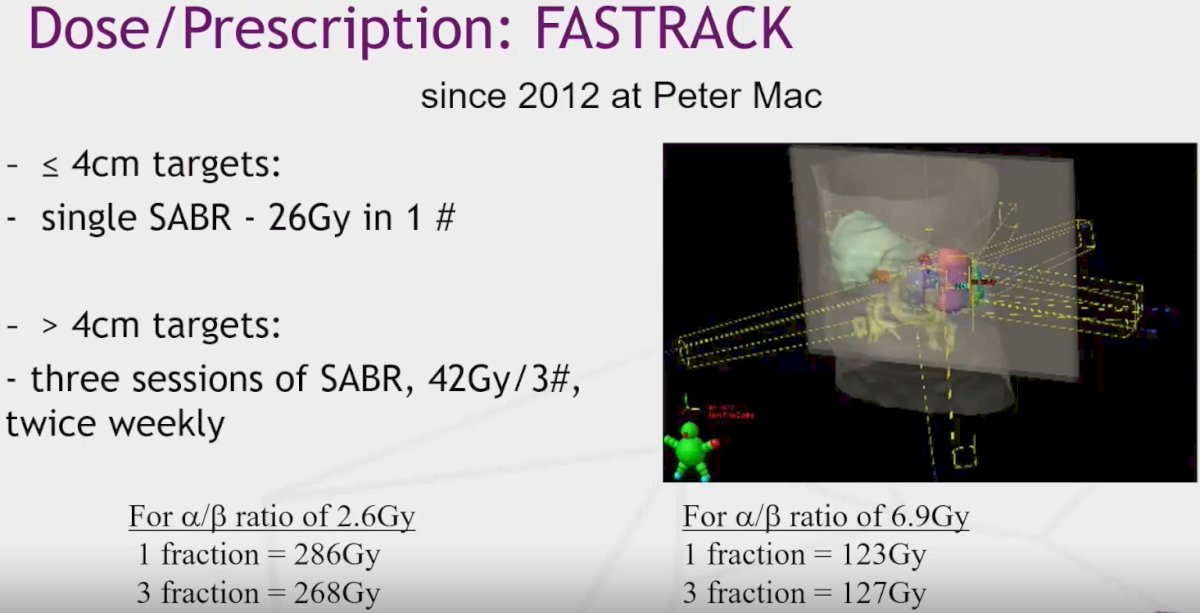
Results of the phase II FASTRACK II trial were presented earlier at this meeting. In the overall cohort of patients treated with SABR (median follow-up of 43 months), the local control rate was 100% with one patient only developing distant failure (freedom from distant failure=99%). The cancer-specific survival is 100%, and the mean kidney function loss was -14.6 ml/min.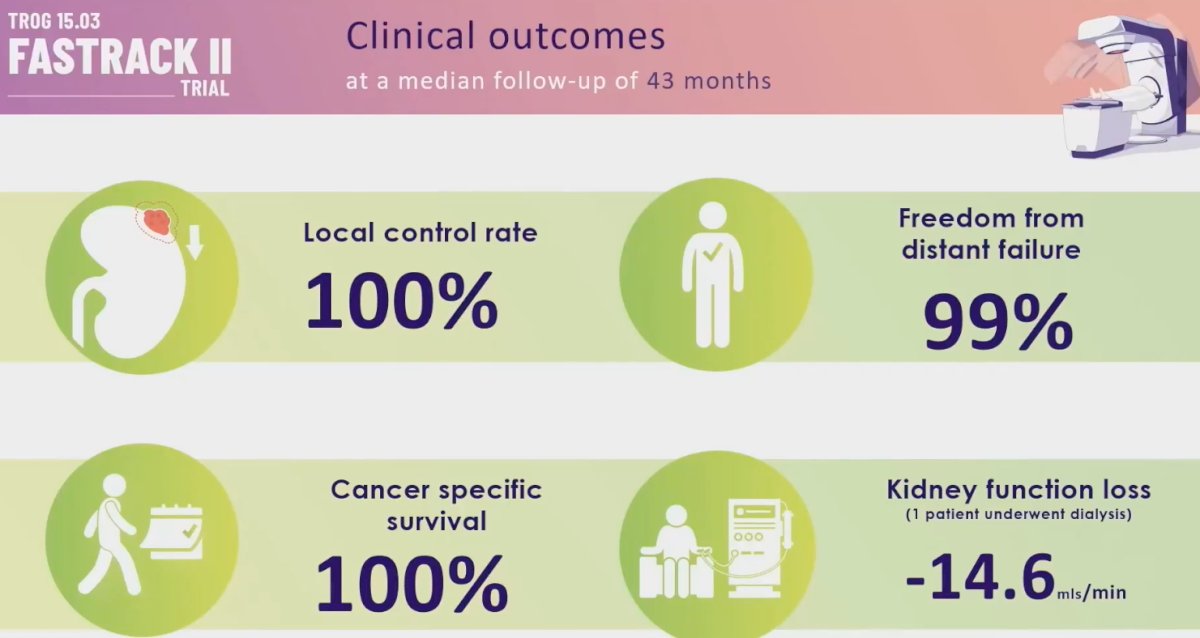
What about renal function post-SABR? In the initial FASTRACK pilot study, Dr. Siva and colleagues performed serial SPECT-CT on patients treated with SABR. As demonstrated below, there was a visible loss in function in high dose-treated regions from 3 months onwards: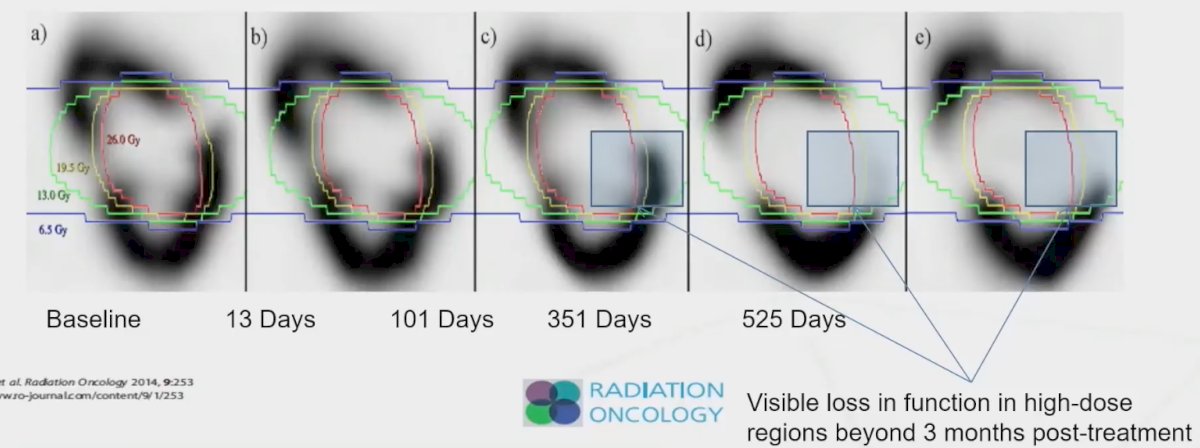
One of the challenges in renal SABR remains response assessment. From a radiologic standpoint, many patients treated with SABR continue to demonstrate serial decreases in tumor size over follow-up, with many patients meeting RECSIT criteria for a ‘partial response’ many years later, as demonstrated in the spider plots below.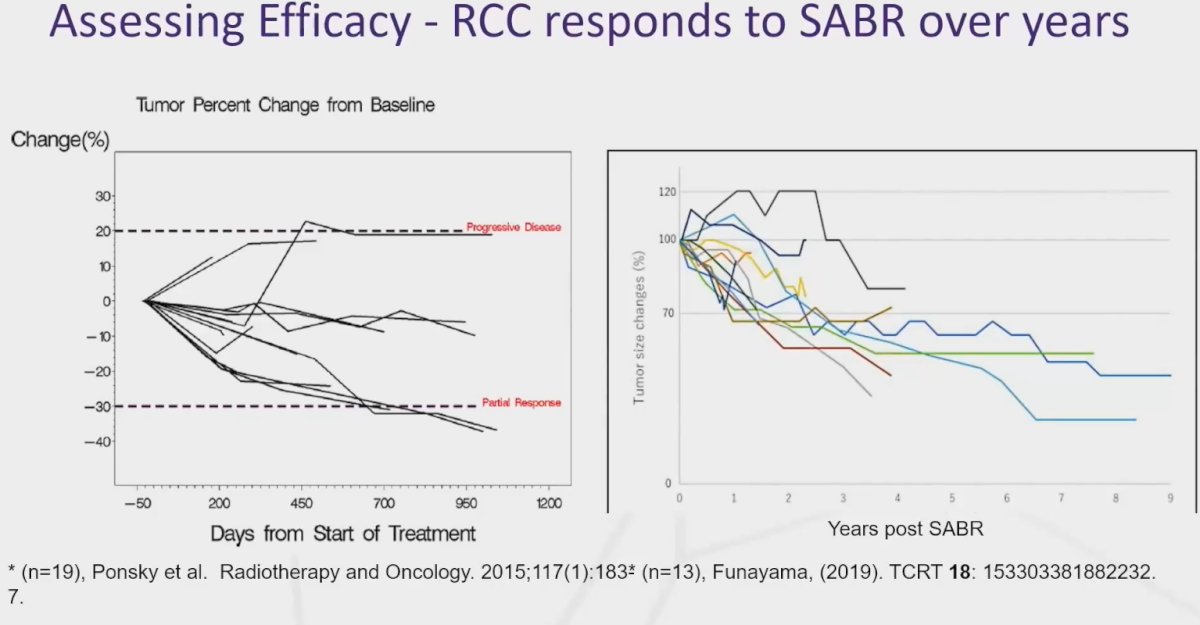
Dr. Siva argued that radiologic assessment with CT contrast enhancement, which is a critical component of response assessment with thermal ablation, is not useful post-SABR. In a single institutional series of 41 patients treated with SABR, 38/41 (93%) had evidence of local control. However, on evaluation of corticomedullary, early nephrographic, and late nephrographic phases, patients had increased enhancement in the post-treatment setting, which is likely related to increased vascular permeability and immune cell infiltration.2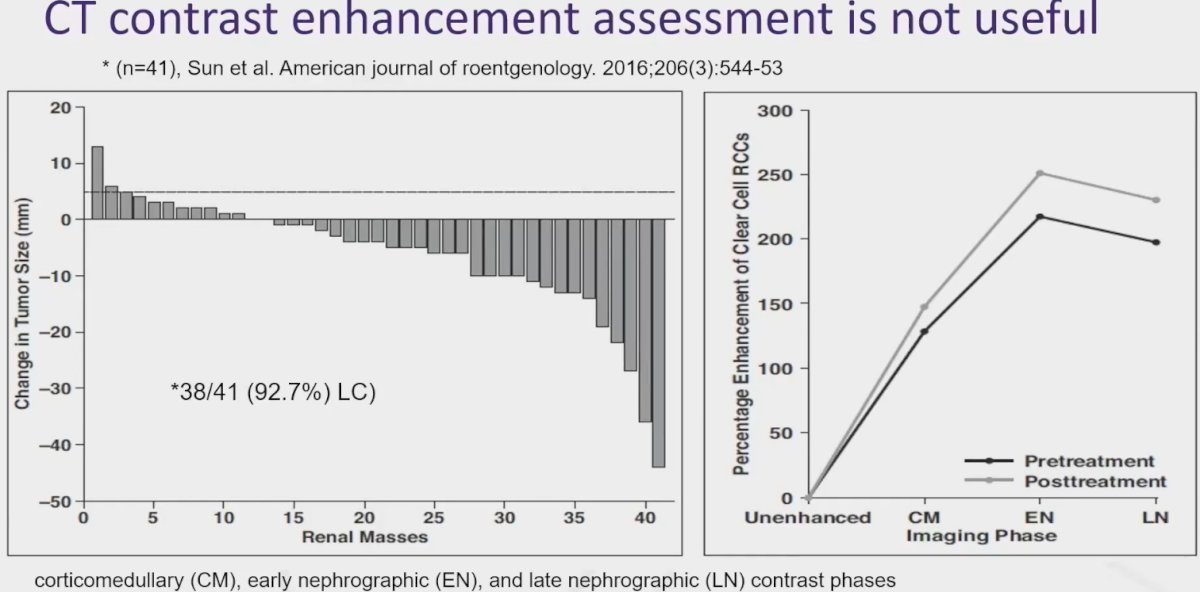
What are some planning tips? Dr. Siva et al. have published the protocol for the recently completed FASTRACK II trial with margins and dose/fractionation constraints for the organs at risk. The only difference to this table below now is that Dr. Siva and colleagues use a planning at risk volume (PRV) for hollow viscus organs, such as the stomach, small bowel, and large bowel, all of which have a 3 mm PRV expansion.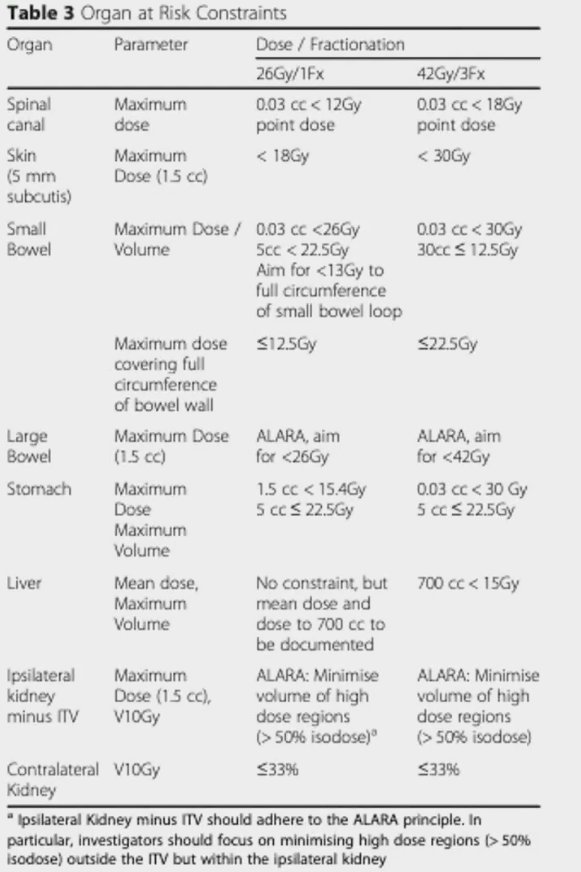
One question that remains unanswered is whether the renal pelvis and calyces are at risk with SABR. This is a concern with thermal ablative procedures, with potential complications such as hypertension, vascular stenosis, and ureteric strictures. However, to date, these have not been consistently reported in the SABR literature.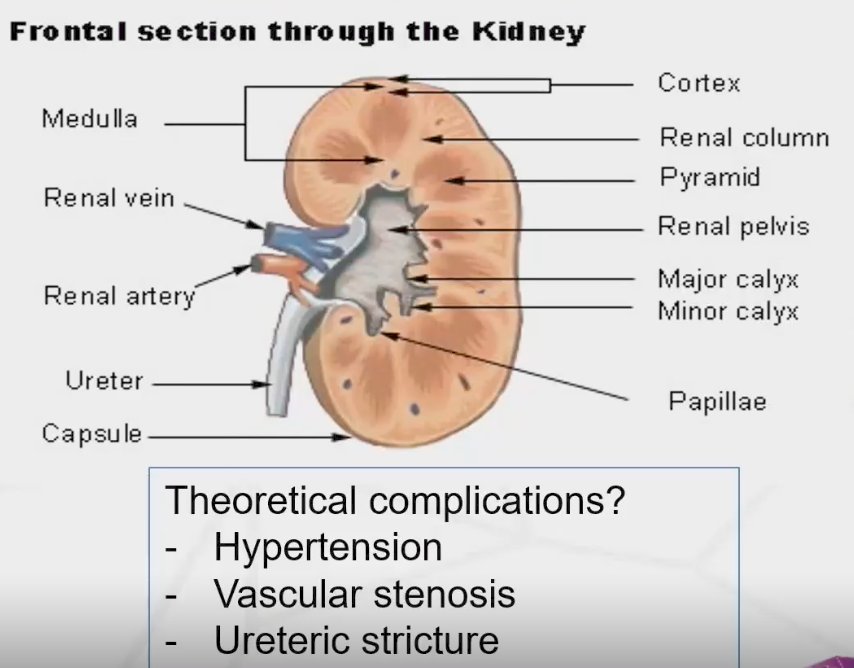
Given that many patients have poor baseline renal function, Dr. Siva recommended that contouring be performed with a slow drip IV contrast protocol to allow for enhanced tumor delineation.
Dr. Siva concluded his presentation with his own planning goals summarized in the slide below:
Presented by: Shankar Siva, PhD, MBBS, FRANZCR, Associate Professor, Peter MacCallum Cancer Centre, Melbourne, Australia
Written By: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 American Society for Therapeutic Radiation Oncology (ASTRO) 65th Annual Meeting held in San Diego, CA between October 1st and 4th, 2023
- Siva S, Pham D, Gill S, et al. An analysis of respiratory induced kidney motion on four-dimensional computed tomography and its implications for stereotactic kidney radiotherapy. Radiat Oncol. 2013;8:248.
- Sun MRM, Brook A, Powell MF, et al. Effect of Stereotactic Body Radiotherapy on the Growth Kinetics and Enhancement Pattern of Primary Renal Tumors. AJR Am J Roentgenol. 2016;206(3):544-53.