
He then moved on to a potential rationale with respect to tumor biology that local therapy may alter the natural history of metastatic disease. This is based on a number of mechanisms including the primary tumor seeding metastatic sites, the primary tumor enhancing metastatic progression, and an immunosuppressive effect of the primary tumor. The first randomized data to support this assertion comes from the recently published trial assessing surveillance or metastasis directed therapy in patients with oligiometastatic prostate cancer following local therapy. They found that metastasis-directed therapy was associated with improved biochemical recurrence free survival and with significant PSA responses. Taken further, for patients with metastatic CRPC, radical prostatectomy was associated with a meaningful decrease in PSA level in approximately 1 in 3 patients.
Highlighting data on molecular profiling of liver metastases in colorectal cancer, Dr. Chapin stressed that molecular characteristics to guide primary therapy in prostate cancer are lacking compared to other tumor sites. However, characterization of primary tumors based on androgen driven, androgen indifferent, and undetermined phenotypes may allow identification of patients with the greatest potential to benefit. Pre-treatment biopsy or serum based assessment of cfDNA may allow for assessment of RB1, PTEN and Tp53 which have demonstrated an association with progression.
Thus, instead of considering all patients with “metastatic prostate cancer” as a homogenous group, Dr. Chapin advocated personalized care based on clinical features, genetic, genomic, and induced responses. Therefore, a role for androgen deprivation therapy, other systemic therapies, chemotherapy, immunotherapy, and local therapy may be integrated for each patient as most appropriate.
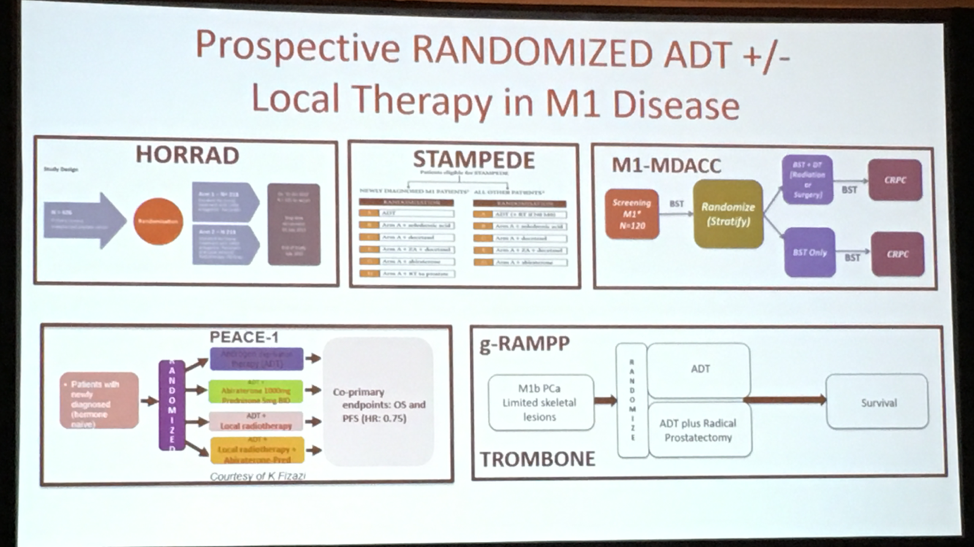
Prior to concluding his talk, Chapin highlighted ongoing trials to assess the role of local therapy, whether surgically or with radiotherapy, in patients with metastatic prostate cancer.
In conclusion, local therapy of patients with metastatic prostate cancer requires prospective, randomized evaluation. Even following this, it is unlikely that such an approach will be beneficial for all patients. Therefore, we need to understand the mechanism of its benefit in order to intelligently integrate multimodal therapy to personalize care.
Presented by: Brian Chapin, MD, FACS The University of Texas, MD. Anderson Cancer Center
Read the Opposing Debate: Treatment of High Risk Advanced and M1 Disease: Is There a Role for Treatment of the Primary? (CON)
Written by: Christopher J.D. Wallis, Urology Resident, University of Toronto @WallisCJD at the 2018 AUA Annual Meeting - May 18 - 21, 2018 – San Francisco, CA USA