Men were prospectively enrolled in a trial of active surveillance with Gleason 3+3=6 or 3+4=7 disease diagnosed in the community. Upon entry into the protocol a confirmatory MRI targeted plus systematic 12 core biopsy were performed to confirm the diagnosis of low or favorable intermediate risk prostate cancer. Patients without cancer detected on confirmatory biopsy or patients with high volume disease were considered eligible for active surveillance. Patient demographics, PSA, prostate volume, PIRADs scores, targeted and sextant biopsy yield, and Gleason scores were recorded upon study enrollment and at the time most recent follow up biopsy.
There were 288 men aged 42-79 years old (mean 62.4) with a mean prostate volume 53.4 ml that satisfied criteria for active surveillance after initial MRI targeted plus systematic biopsy. All patients demonstrated Gleason 3+3=6 (73%) or Gleason 3+4=7 (27%) disease upon study enrollment. Over a mean follow up of 32.6 months (3.2-109.3 months), 35.1% demonstrated Gleason Score upgrading and 14.6% (n=42) of patients were upgraded to 4+3=7 or higher disease on repeat MRI targeted fusion plus systematic biopsy. On a per year basis, this translated to a 4.8% rate of any upgrading, and a 2.3% rate of upgrading to clinically significant (Gleason Score =4+3) disease per year.
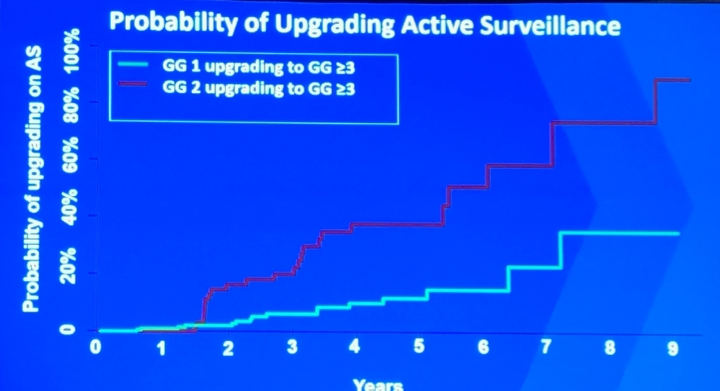

Rates of upstaging appear to level off at approximately 5 years of follow up. However, these patients should likely be monitored for a longer duration considering that intervention/upgrading of patients on active surveillance from the University of Toronto levelled off at 15-20 years1.
Dr. Lebastchi made the following concluding remarks:
- Upgrading to GG >=3 occurs more commonly if the patient was enrolled with GG2 disease
- Within the first 5 years, upgrading to GG >= 3 occurs more rapidly among patients with GG2 patients compared to GG1
- Of these upgrading events, 2.3% per year will represent upgrading to clinically significant disease.
- The role of mpMRI and targeted biopsy is not well understood on active surveillance
- Continued work is needed to define the best management options
Co-Authors: Amir H. Lebastchi, Johnathan Bloom, Patrick Gomella, Sandeep Gurram, Thomas Sanford, Johnathan DiBianco, Samuel Gold, Graham R. Hale, Sherif Mehralivand, Vladimir Valera Romero MD, Maria Merino, Bethesda, MD, M. Minhaj Siddiqui, College Park, MD, Peter L. Choyke, Brad Wood MD, Howard Parnes, Barris Turkbey, Peter A. Pinto, Bethesda, MD
Written By: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University - Medical College of Georgia @zklaassen_md at the American Urological Association's 2019 Annual Meeting (AUA 2019), May 3 – 6, 2019 in Chicago, Illinois
Reference:
1. Klotz L, Vesprini D, Sethukavalan P, et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol 2015;33(3):272-277.