(UroToday.com) The 2024 American Urological Association (AUA) Annual Meeting held in San Antonio, TX was host to a non-invasive bladder cancer podium session. Dr. Yair Lotan presented the development and validation analysis of an artificial intelligence-powered pathology assay for predicting response to intravesical BCG in high-risk, non-muscle invasive bladder cancer (NMIBC).
Dr. Lotan noted that existing clinicopathologic models overestimate the risk of recurrence and progression in NMIBC patients.

Potential implications of an accurate recurrence/progression risk predictor tool in BCG-treated NMIBC patients may include the following:
- Selection of optimal candidates for BCG versus emerging non-BCG therapies (e.g., Gemcitabine/Docetaxel, TAR200, BCG + Pembrolizumab)
- Identifying patients least likely to benefit from BCG in the era of BCG shortages
- Determining which patients are at the highest risk of progression and, therefore, candidates for early cystectomy
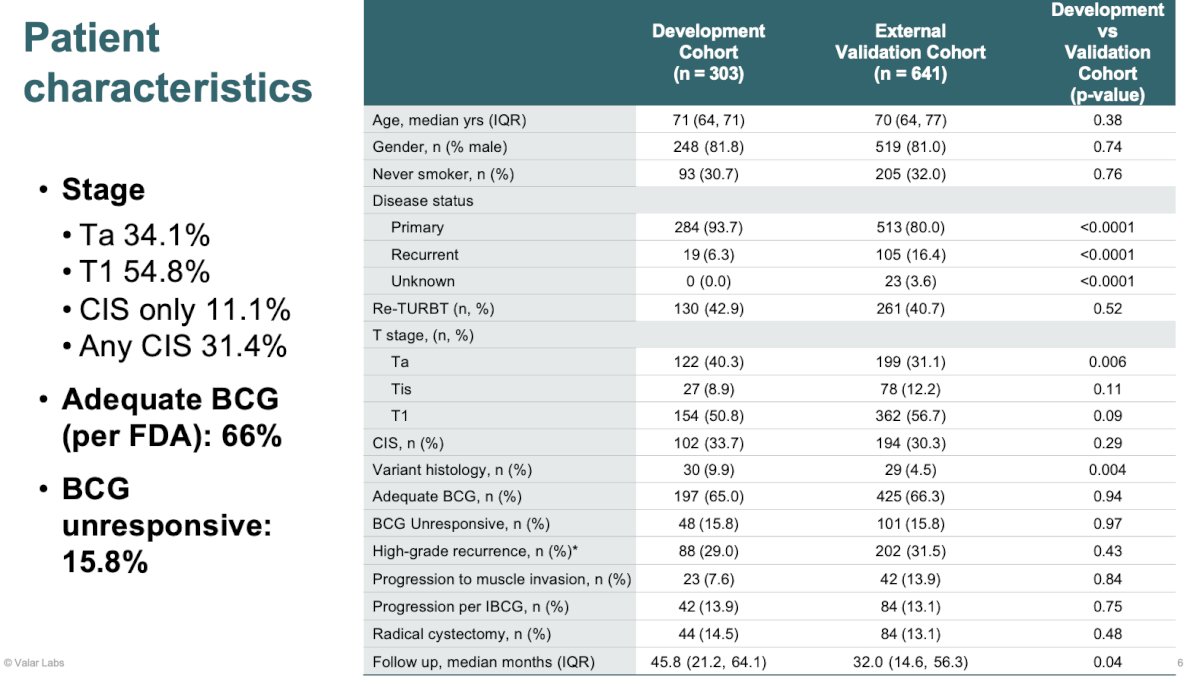
In this study, Dr. Lotan and colleagues developed and validated a computational histologic artificial intelligence (CHAI) assay using a cohort of 944 patients with high-risk, BCG-naive NMIBC treated with BCG from 12 centers. All patients underwent TURBT +/- restaging TURBT followed by intravesical BCG. This cohort was split into development (n=303) and external validation cohorts (n=641). Two digital H&E whole slide images were obtained from TURBT for each patient. Patients meeting the following criteria were excluded:
- Inadequate pathologic tissue
- Induction/maintenance with non-BCG treatments post-TURBT
- Muscle invasive, node positive, or metastatic disease

Patient characteristics are summarized below. 55% of patients had T1 disease and any CIS was present in 31.4% of patients. 66% of patients received adequate BCG (per FDA criteria). 16% were deemed BCG unresponsive.
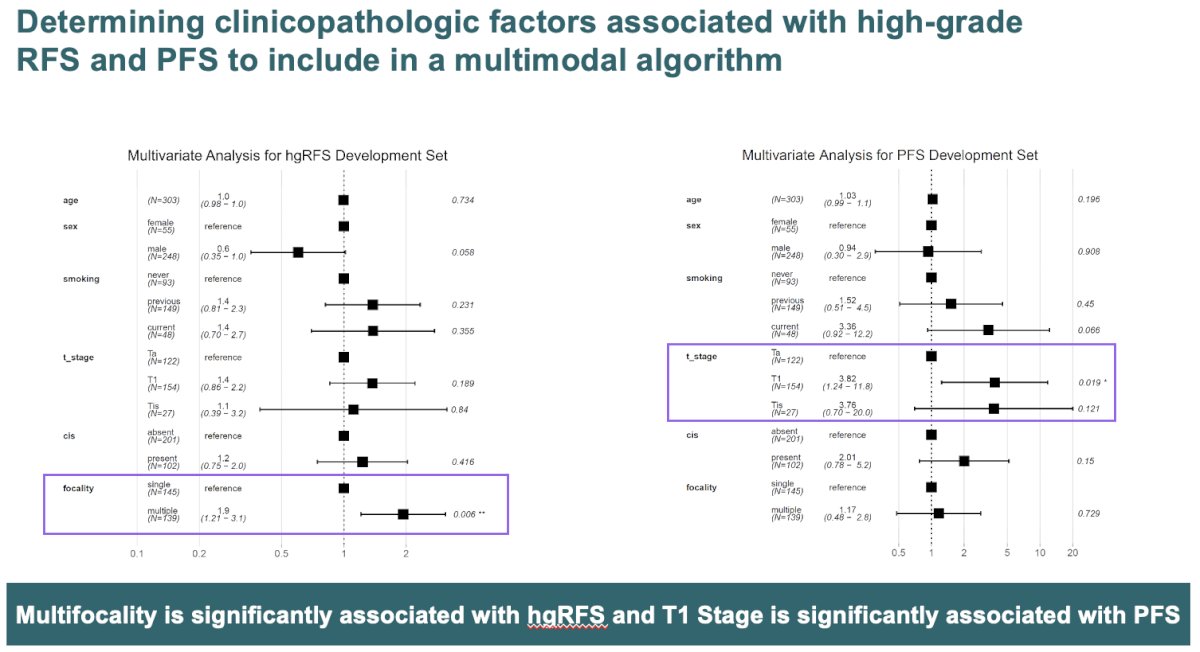
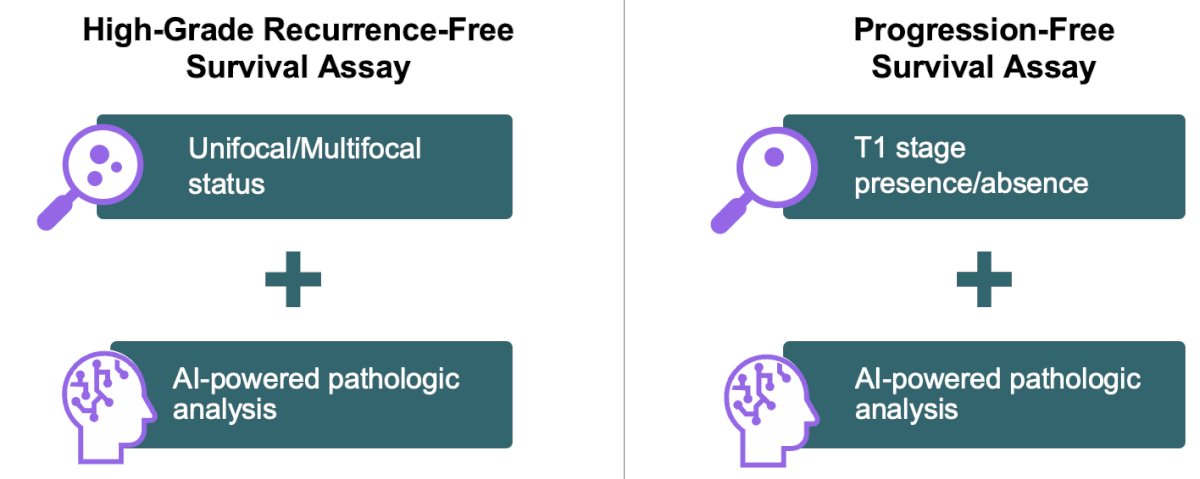
First, the investigators evaluated the clinicopathologic factors associated with high-grade recurrence-free and progression-free survivals to include in the multimodal algorithm. They identified multifocality as a significant risk factor for high-grade recurrence and T1 stage as being significantly associated with the risk of progression.
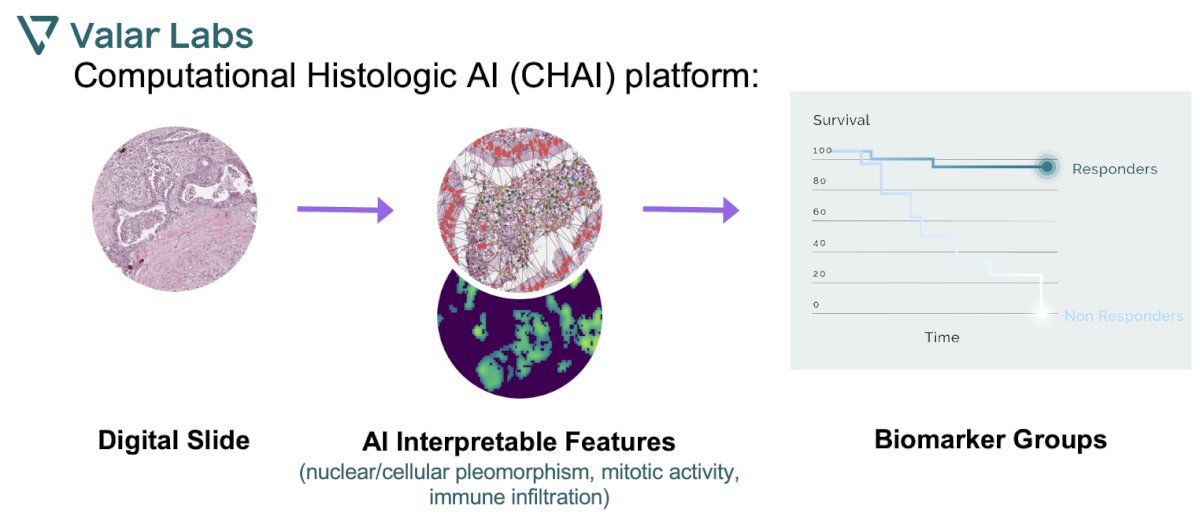
Next, the AI algorithm was trained on the development set to quantify morphologic features which were combined with clinicopathologic characteristics to create a multimodality assay:
The CHAI assay was “locked” after training on the development set:
Multivariable analysis demonstrated that the computational histology AI assay was associated with high-grade recurrence-free and progression-free survivals independently of clinicopathologic factors.

When the CHAI assay was compared to the EORTC 2016 risk scoring model for stratifying recurrence-free survival in the validation cohort, it demonstrated superior discriminatory performance:
- EORTC shows unstable prognostication with the crossover of group survival plots
- Patients in CHAI RR-High group have a two-fold higher rate of high-grade recurrence-free survival post-BCG, compared to those in the CHAI RR-Low group (HR = 2.1 [95% CI 1.8, 2.4], p<0.0001).

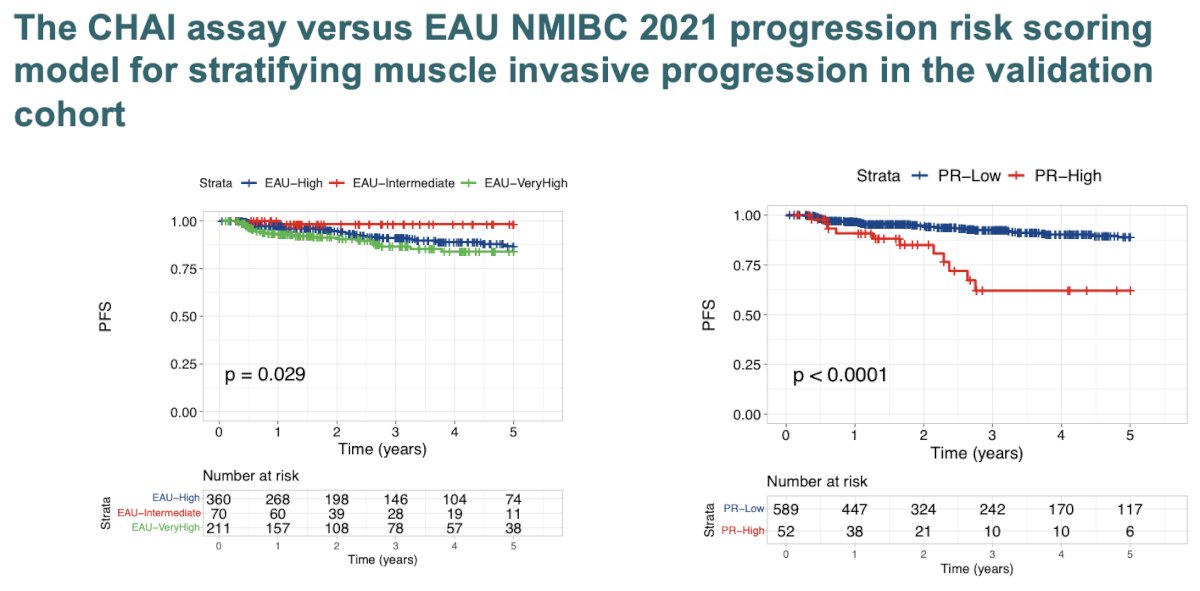
Similarly, the CHAI assay demonstrated superior discriminatory performance compared to the EAU NMIBC 2021 progression risk scoring model for stratifying muscle invasive progression in the validation cohort. Patients in the CHAI assay PR-High group demonstrated a 3-fold higher risk of progression post-BCG, compared to the PR-Low group (HR = 3.9 [95% CI 2.8, 5.4], p<0.001).
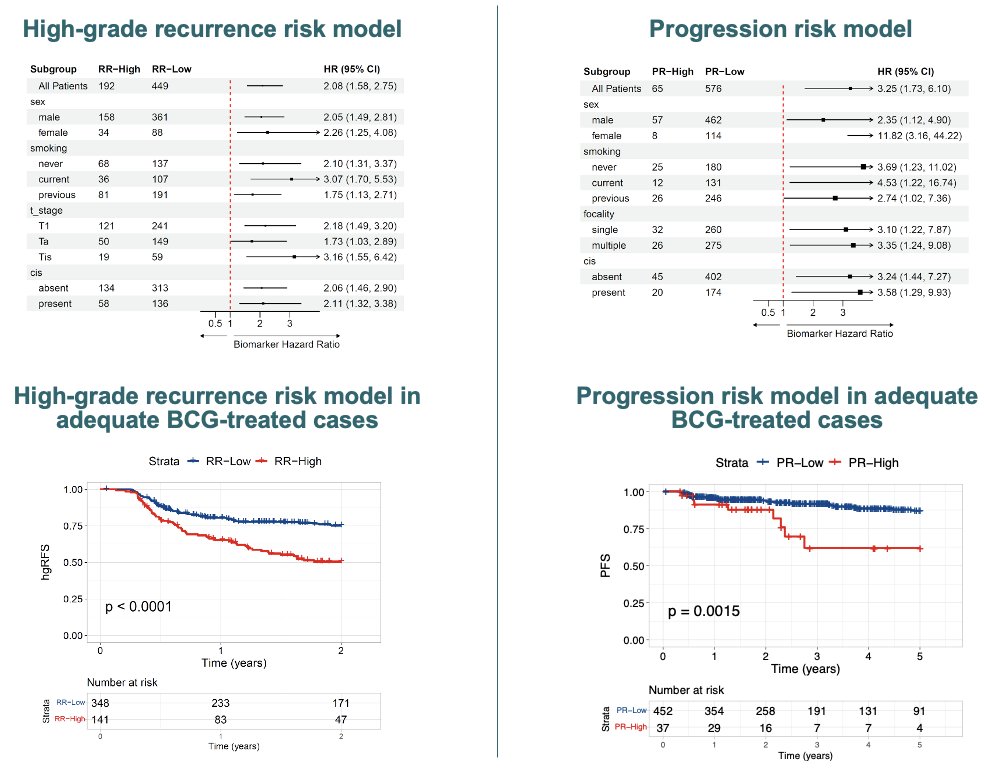
Significantly, the CHAI assay maintained performance across clinical subgroups and in patients receiving adequate BCG in the validation cohort. The AI model performance was maintained across clinical subgroups. In patients treated with FDA-defined adequate BCG, the AI model sustains performance:
- RR-High vs RR-Low at 2 years (HR 2.2 [95% CI 1.9, 2.6], p<0.0001)
- PR-High vs PR-Low at 3 years (HR 3.2 [95% CI 2.2, 4.8] p<0.003)
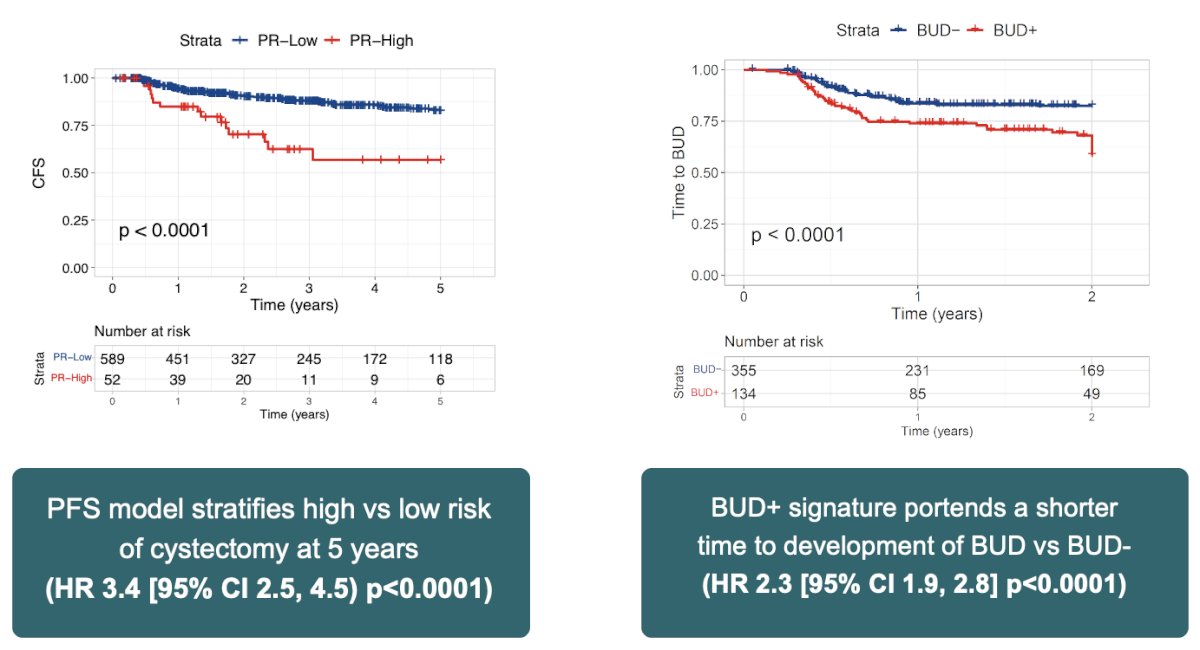
The CHAI assay furthermore identifies cases at high risk of cystectomy and BCG unresponsive disease in the validation cohort:
Dr. Lotan concludes with the following take home messages and clinical implications:
Workflow advantages:
- In contrast to genetic testing, this AI model avoids issues of “inadequate tissue” and avoids a 2–4 week turnaround, with results available in 2-3 days
- Can be leveraged by any hospital (academic or community) globally using tissue from TURBTs
- Arms clinicians with nuanced data to help guide treatment selection and patient counseling regarding alternative treatment approaches
- Better places clinicians for clinical decision-making in an era of BCG shortage and when novel therapies or therapeutic combinations become available since this assay could help identify patients less likely to benefit from BCG
- This may have implications for tumor surveillance regimens
Presented by: Yair Lotan, MD, Professor, Chief of Urologic Oncology, University of Texas Southwestern Medical Center, Dallas, TX
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 American Urological Association (AUA) Annual Meeting, San Antonio, TX, Fri, May 3 – Mon, May 6, 2024.
Related content:
AI-Based Assessment Tool for Predicting BCG Response in Bladder Cancer Patients - Yair Lotan
Leveraging AI Biomarkers to Navigate the Evolving Landscape of Bladder Cancer Treatment - Stephen Williams