(UroToday.com) The third day of the American Urological Association Annual Meeting featured an intriguing poster session on stone disease. During this session, Mr. Karan Thaker from the University of California, Los Angeles, and colleagues presented research on bacteria and calcium oxalate (CaOx) stone formation.
Although it has been previously estimated that 80% of kidney stones consist of calcium oxalate, stone pathogenesis remains poorly understood. Prior research has suggested that bacteria, including Escherichia coli and Pseudomonas aeruginosa, are associated with the development of nephrolithiasis through biofilm accumulation. Accordingly, Mr. Thaker and colleagues aimed to assess the role of uropathogens in initiating biofilm formation, bacterial pathways for stone formation, and the relationship between biofilm-forming bacteria and CaOx crystals.
To visualize the 3-dimensional nature and underlying configuration of human uroliths, researchers utilized high-resolution X-ray microscopy (microtomography/micro-CT) and X-ray fluorescence microscopy (micro-XRF). Additionally, in-vitro CaOx crystallization with artificial urine, in the presence and absence of E. coli and P. aeruginosa, was conducted. Crystal size, morphology, and formation kinetics were assessed using confocal and scanning electron microscopy (SEM). Furthermore, Raman (RS) and Energy Dispersive X-ray Spectroscopy (EDAX) were employed to analyze the chemical composition of the resultant CaOx. Notably, the research team developed a microfluidic kidney model to simulate urinary tract physiology.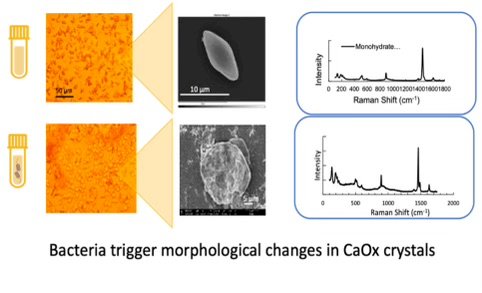
Overall, stones exhibited a complex 3D morphology composed of stratified construction, with both organic and inorganic layers resembling biomineralization. Porosity was present in each individual section. SEM analysis revealed substantial disparities in crystal morphology between crystals influenced by bacteria and control samples, with rapid clustered aggregation of crystals mediated by E. coli (as seen in the image above). Subsequent RS and EDAX analyses confirmed the composition of these crystals as predominantly consisting of calcium oxalate (CaOx). Additionally, Pseudomonas aeruginosa facilitated a notable augmentation in the size of CaOx crystals by up to 280% within a 10-day period, exhibiting a growth rate 250% higher than that of control conditions. Furthermore, the microfluidic kidney model illustrated that secretions from P. aeruginosa and E. coli significantly bolstered the crystallization, expansion, and aggregation of CaOx compared to control scenarios.
In their closing statements, Mr. Thaker et al. underscored several significant findings. They emphasized that renal calculi exhibit patterns reminiscent of biomineralization, shedding light on the intricate nature of stone formation. Moreover, their research unveiled the substantial impact of secretions from biofilm-forming bacteria on the development and aggregation of calcium oxalate (CaOx) crystals in vitro, highlighting the role of bacterial activity in stone formation. Looking ahead, the team outlined future research directions, including the structural analysis of high-resolution data and the investigation of bacterial-induced crystallization mechanisms through bacterial mutation assays. These insights pave the way for deeper understanding and potential breakthroughs in the prevention and management of kidney stone formation.
During the question-and-answer session, an audience member queried Mr. Thaker about the choice of E. coli over other bacterial species, given the prevalent association of calcium oxalate with metabolic stones. Mr. Thaker referenced recent studies analyzing patient stone samples, which identified E. coli and Pseudomonas as common bacteria found in stones from patients without positive urine cultures. In response, Dr. Joseph Crivelli inquired about Mr. Thaker’s team's plans to test other bacterial species, including gram positives, to which Mr. Thaker clarified that they had solely selected these strains based on recent research findings. When asked about the mechanism behind the formation of crystal aggregations, whether from biofilm secretions or bacterial structure, Mr. Thaker conceded that the exact process remains unclear. However, he outlined several theories proposed by the team, noting that bacterial-influenced crystals exhibited central rough etchings and increased surface aggregation, leading to erratic connections between crystals (as seen in the image below).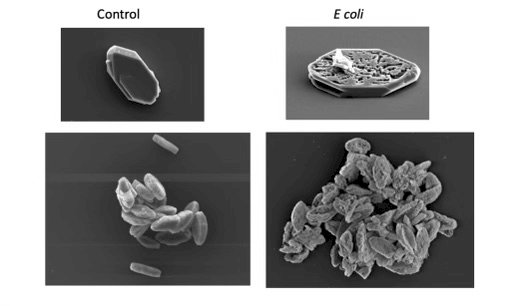
Additionally, scanning electron microscopy revealed a hollowed-out interior in the bacteria-influenced crystals, suggesting a possible explanation for their propensity to grow into one another at odd angles, distinct from the smooth, side-by-side stacking observed in control crystals. These insights represent significant steps toward unraveling the complex dynamics of bacterial involvement in crystal aggregation formation.
Presented by: Karan Thaker, Research Student, University of California, Los Angeles
Written by: Mariah Hernandez, Department of Urology, University of California, Irvine, @mariahch00 on Twitter during the 2024 American Urological Association (AUA) Annual Meeting, May 3 — May 6, 2024, San Antonio, Texas
References:
- Evan AP. Physiopathology and etiology of stone formation in the kidney and the urinary tract. Pediatr Nephrol. 2010;25(5):831-841.
- Tavichakorntrakool R, Prasongwattana V, Sungkeeree S, et al. Extensive characterizations of bacteria isolated from catheterized urine and stone matrices in patients with nephrolithiasis. Nephrol Dial Transplant. 2012;27(11):4125-4130.