(UroToday.com) The 2024 American Urological Association (AUA) annual meeting held in San Antonio, TX between May 3 and May 6, 2024, was host to the advanced kidney cancer podium session (PD18). Dr. Daniel Shapiro presented the results of a multicentric retrospective study using data from metastatic renal cell carcinoma (mRCC) patients who underwent cytoreductive nephrectomy (CN) at 8 institutions and explored the survival outcomes among patients with metastatic sarcomatoid (msRCC) treated with either targeted therapy (TT) or immune checkpoint inhibitors (IO) aiming to determine if the sequence of CN and systemic therapy was associated with survival.
Dr. Shapiro opened his presentation by noting that renal cell carcinoma with sarcomatoid dedifferentiation is relatively common in mRCC, with sarcomatoid features present in up to 20% of these patients. Historically, these features have been associated with a poor prognosis, with an estimated 5-year overall survival (OS) of approximately 23%. However, the landscape has shifted with the advent of immunotherapy, as evidenced by the CheckMate 214 study. In this trial, patients with mRCC experienced remarkable outcomes, with a notable complete response rate of 23%, and a threefold increase in median OS when treated with ipilimumab + nivolumab compared to sunitinib.1 Given the improved survival observed with immunotherapy, the investigators sought to explore the optimal timing for cytoreductive surgery among patients with mRCC.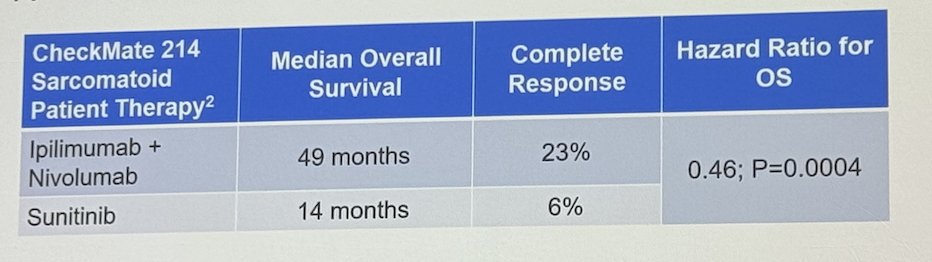
The investigators identified a total of 1,421 patients with mRCC who underwent CN. Among them, 309 (22%) exhibited sarcomatoid features in surgical pathology. Patients were stratified into four cohorts based on the type of systemic therapy they received and the sequence of treatments:
- Upfront IO+ deferred CN (IO+CN)
- Upfront targeted therapy + deferred CN (TT+CN)
- Upfront CN + deferred IO (CN+IO)
- Upfront CN + deferred targeted therapy (CN+TT)
This analysis focused on the 309 patients with sarcomatoid features. Their median age was 61 years, with 71% being male, and the majority had clear cell RCC subtype (77%). The median follow-up period was 37 months. Dr. Shapiro elaborated that they compared the sarcomatoid cohort (n=309) to a cohort of 1,112 patients with mRCC without sarcomatoid features who underwent CN. Clinical and demographic characteristics are shown in the table below.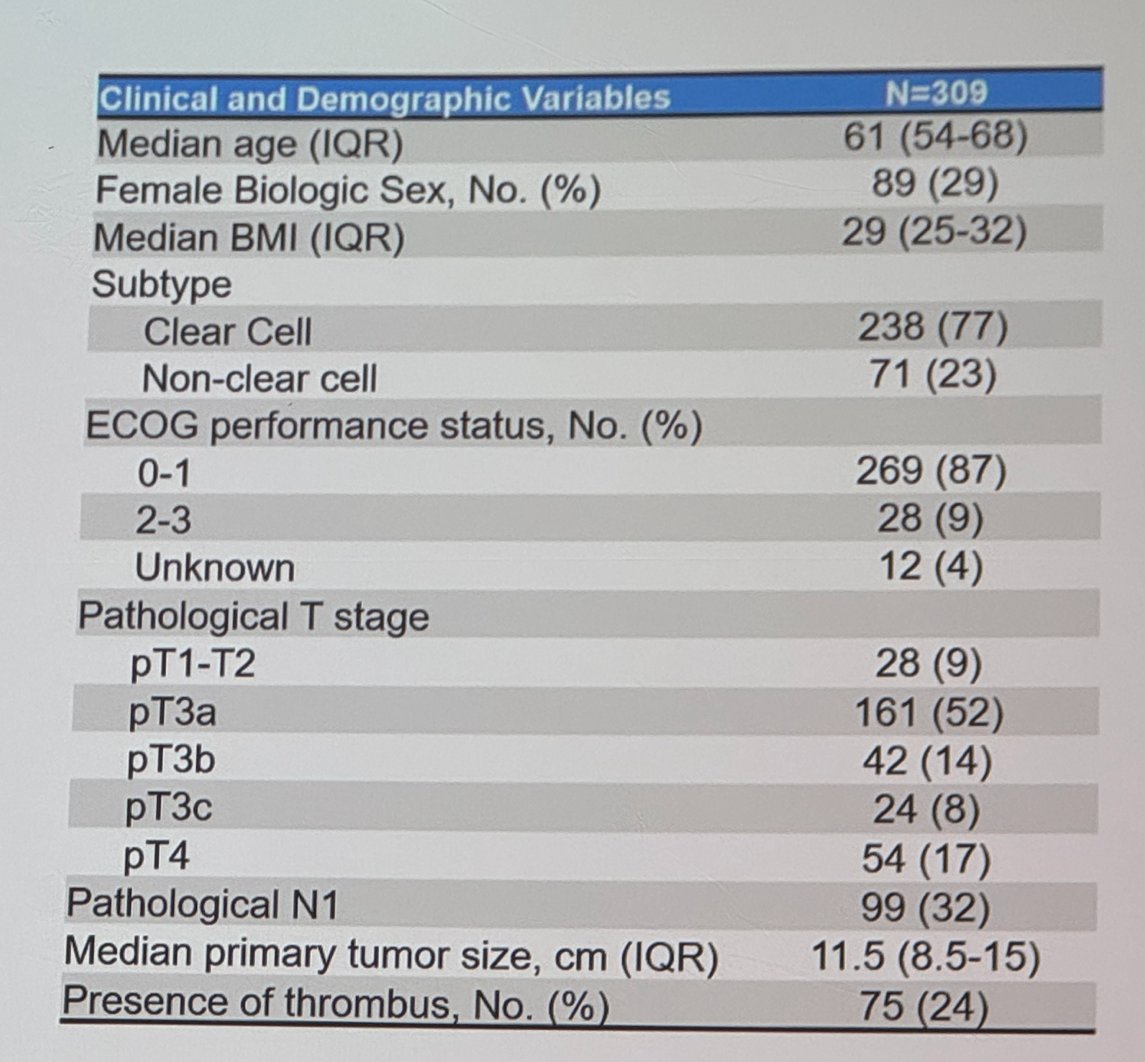
Dr. Shapiro showed that in their study, patients with sarcomatoid features exhibited significantly worse overall survival (median 15 vs. 37 months, p < 0.001). Furthermore, patients treated with IO therapy demonstrated significantly improved OS compared to those not treated with IO (median 40 vs. 13 months, p = 0.0001), a finding corroborated by multivariable Cox regression analysis (HR 0.4; 95% CI 0.3-0.6).
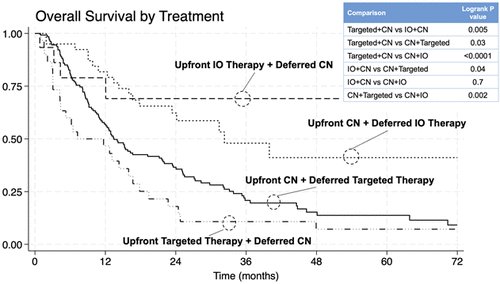
Furthermore, he elaborated on the treatment sequence in patients with sarcomatoid features. Among them, 60% underwent upfront CN+TT, 19% underwent upfront CN+IO, 14% underwent upfront TT+CN, and 7% underwent upfront IO+CN. Patients receiving IO therapy at any time point exhibited significantly improved OS compared to those not receiving IO. Among patients receiving TT, upfront CN was linked with reduced mortality (HR 0.6; 95% CI 0.4-0.9, p = 0.03) adjusting for age, metastatic burden, ECOG PS, and pT stage. However, among patients who received IO therapy, the sequence of systemic therapy and CN did not correlate with survival (p = 0.7).
To wrap up, he acknowledged the limitations of the study, including its retrospective nature which could be influenced by surgical selection bias.
Dr. Shapiro concluded his presentation with the following key points:
- IO therapy has significantly improved overall survival for mRCC patients with sarcomatoid features.
- Among patients with mRCC, the timing of IO therapy did not correlate with OS. However, among patients treated with targeted therapy, upfront CN was associated with improved OS.
Presented by: Daniel Shapiro, MD. Urologic Oncologist, University of Wisconsin-Madison, Madison, WI
Written by: Julian Chavarriaga, MD - Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @chavarriagaj on Twitter during the 2024 American Urological Association (AUA) annual meeting held in San Antonio, TX between May 3rd and May 6th, 2024
Reference: