(UroToday.com) The 2024 American Urological Association (AUA) annual meeting held in San Antonio, TX between May 3 and May 6, 2024, was host to the advanced prostate cancer moderated poster session. Dr. Hsin-Ho Shih presented the results of a retrospective cohort of patients who started androgen deprivation therapy (ADT) and androgen receptor pathway inhibitors (ARPI) for de novo metastatic hormone-sensitive prostate cancer (mHSPC). They explored if the time to nadir (TTN) PSA and a deep PSA response was associated with predicting oncological outcomes.
Dr. Hsin-Ho Shih began his presentation by explaining that TTN PSA has been previously known as a predictive factor after initiation of ADT and ARPI. Rapid decline in PSA and deep PSA response are believed to be associated with superior oncological outcomes and prognosis. They used a retrospective cohort of 144 patients with de novo mHSPC who started ADT plus an ARPI. Patient characteristics are shown below in Table 1.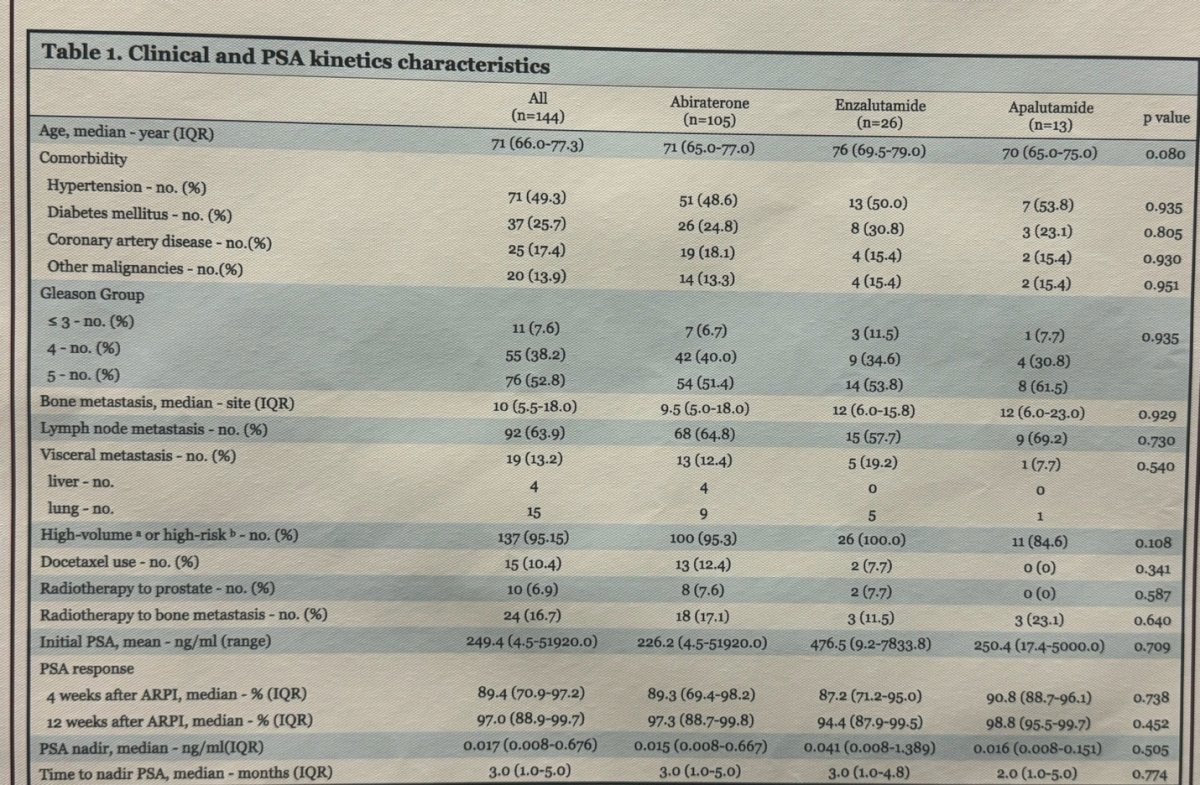
The definitions used for this study were:
- Time to nadir (TTN): Time from ARPI initiation to PSA nadir or reaching a PSA level < 0.2 ng/ml.
- Deep PSA response: PSA <0.2 ng/ml.
The presenter showed that in this retrospective cohort, the median PSA nadir was 0.017 ng/ml, and 67.4% of patients achieved a deep PSA response. Interestingly the time to achieving an A ≥ 50% reduction in PSA from baseline (PSA50), 90% or 99% varied depending on the ARPIs used in this study. (Figure below)
Attaining a deep PSA response correlated with a reduced risk of PSA progression (HR 0.049, 95% CI 0.018-0.131, p<0.001). The median TTN was 3 months. However, they observed that while achieving a deep PSA response was linked to a lower risk of progression, reaching a median TTN in ≥ 3 months did not decrease the risk of PSA progression (HR 0.470, 95% CI 0.217-1.017, p=0.06) compared to those whose TTN was < 3 months.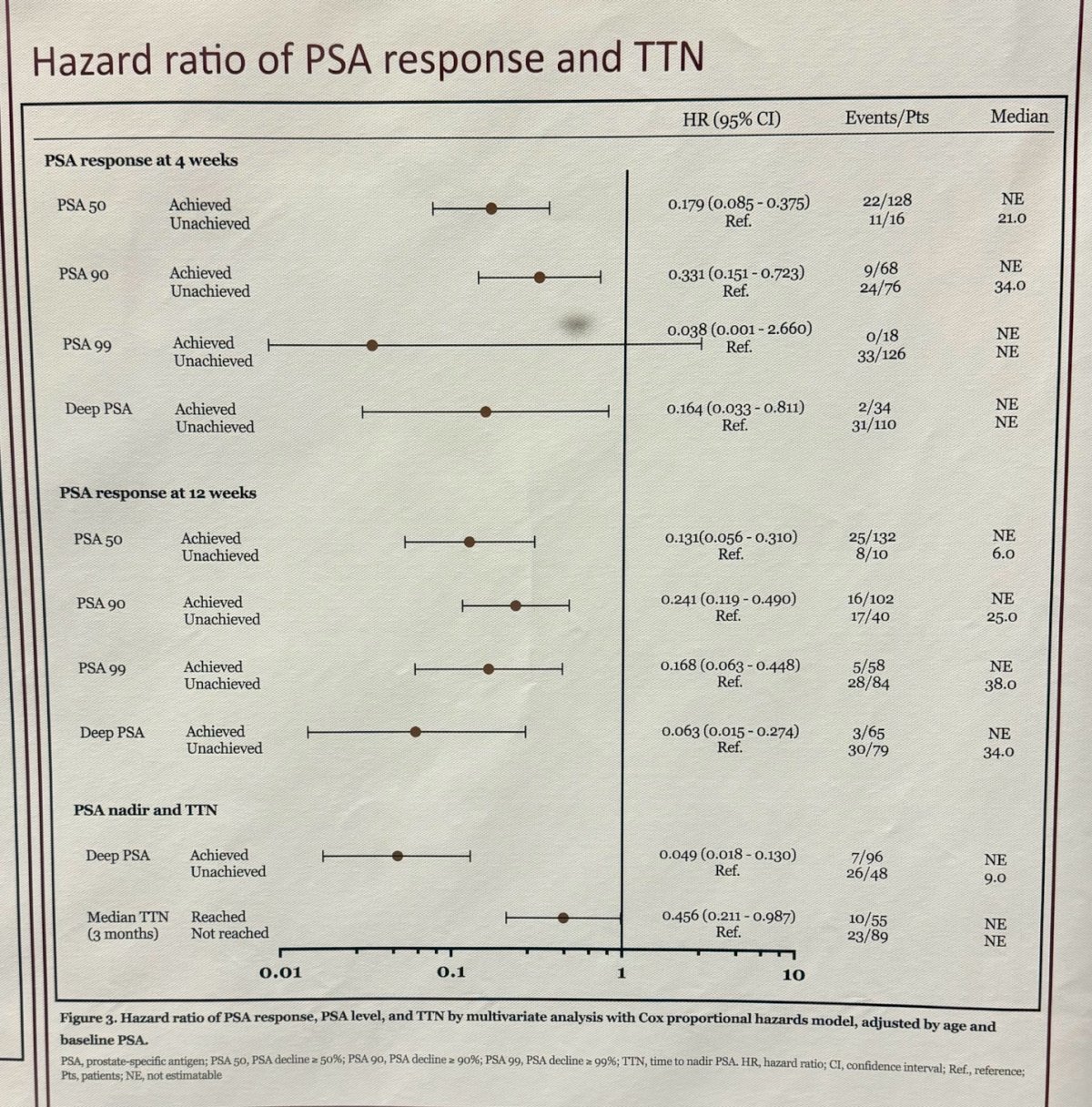
In an exploratory analysis, they found that the group of patients who neither achieved a deep PSA response nor had a TTN <3 months had a significantly lower 2-year PSA progression-free survival (0% vs. 55%, p<0.001) compared to the group without a deep PSA response but whose patients achieved nadir in less than 3 months. 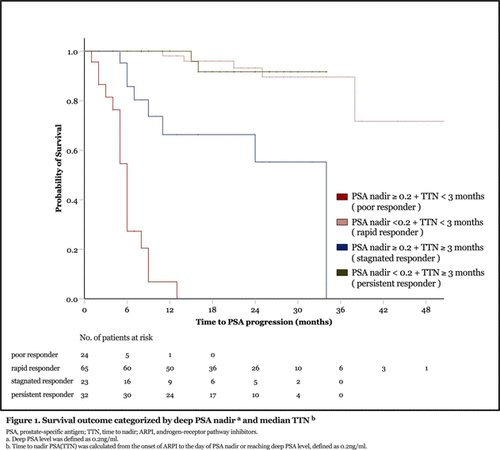
Dr. Hsin-Ho Shih ended his presentation concluding that achieving deep PSA nadir (<0.2 ng/ml) was a reliable predictor of PSA progression-free survival, while TTN showed good predictive efficacy only if deep PSA response was not achieved. Patients with TTN less than 3 months showed different PSA-progression-free survival outcomes based on their PSA nadir level.
Presented by: Hsin-Ho Shih, MD, Professor, Harbin Institute of Technology, Harbin, China
Written by: Julian Chavarriaga, MD - Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @chavarriagaj on Twitter during the 2024 American Urological Association (AUA) annual meeting held in San Antonio, TX between May 3rd and May 6th, 2024