Ideal candidates for radical TURBT include those that have (i) cT2 tumors < 3cm, (ii) no residual tumor on re-TURBT, (iii) no concomitant CIS, and (iv) no hydronephrosis/no upper tract lesions. However, Dr. Van der Heijden cautions that this is very controversial whether this treatment is oncologically safe and should only be performed in patients not fit for more aggressive treatments. Ideal partial cystectomy patients may include those with (i) solitary tumors < 5cm, (ii) excision where a 2cm margin is possible, (iii) no concomitant CIS, and (iv) no hypercontractility of the bladder. Dr. Van der Heijden also notes that only ~5% of patients actually fit the above criteria.
Dr. Van der Heijden then discussed external beam radiation therapy, stating that for nearly 50 years radiotherapy has been used as monotherapy in some patients with MIBC. These were typically patients with inoperative MIBC and most underwent a TURBT prior to radiotherapy (ie. bimodal therapy). Previous studies have shown that the 5-year OS in cT2 patients is 27-59% and 10-38% 5-year OS for cT3 patients. Patients receiving radiotherapy typically receive 55-66 Gy, however higher doses improve long-term local control. Dr. Van der Heijden does caution that higher radiotherapy doses increase toxicity, including hematuria, urinary and fecal urgency, abdominal complaints, and fatigue. Similar to radical TURBT, this should only be offered to patients that are not fit for more aggressive treatment.
Interstitial brachytherapy has also been combined with EBRT boost to the primary tumor. These ideal candidates include those with (i) solitary bladder tumors <5 cm, (ii) stage T1 to T3a, and (iii) no concomitant CIS. Van der Steen-Banasik et al. performed a case control study in which cT1 patients underwent TURBT + EBRT 4 fractions 4.5 Gy + brachytherapy 60 Gy, and cT2 patients underwent either radical cystectomy or TURBT + EBRT 20 fractions 2 Gy + brachytherapy 30 Gy [1]. For patients in the cT2 arm, there was no difference in survival outcomes between the cystectomy group and TURBT/EBRT/brachytherapy group: 10-year OS was 33% in the brachytherapy group vs 42% in the cystectomy group (p=0.70), and 10-year DSS was 66% in the brachytherapy group vs 57% in the cystectomy group (p=0.12). Dr. Van der Heijden concluded that based on this literature, this brachytherapy-based treatment option may be considered in cT1-2 tumors, as the limited OS results are comparable to radical cystectomy.
Recently, trimodal therapy has been prominent in the literature as a bladder preservation technique for MIBC [2-4]. The ideal candidates for trimodal therapy include those with (i) small solitary tumors, (ii) complete TURBT, (iii) early clinical stage T2-T3a, (iv) no concomitant CIS, and (v) no hydronephrosis. With these strict criteria, only 6-19% of patients with MIBC fit these criteria. Two strategies for trimodal treatment:
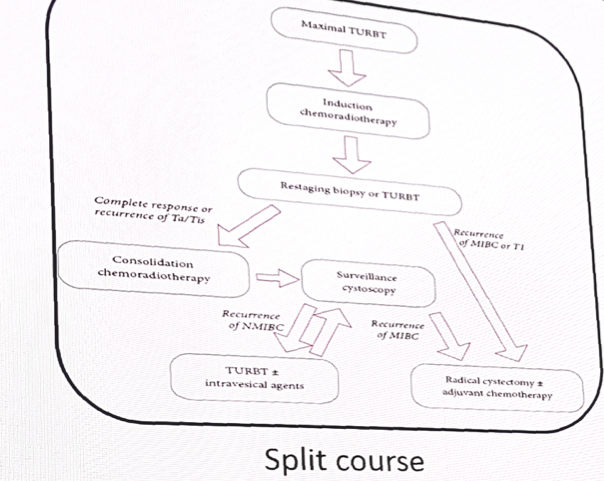
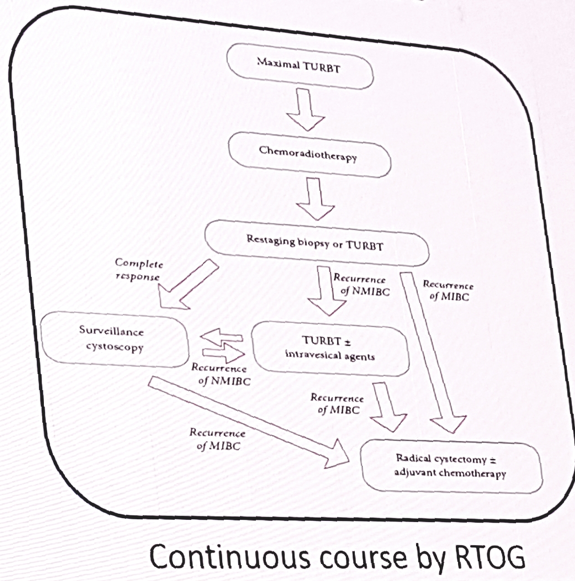
In the largest institutional experience (n=348) to date with split course trimodal therapy from Massachusetts General Hospital, the 5-year OS rate is 52%; cT2 is 61% and cT3-T4 is 41% [3]. In the largest series of continuous chemotherapy per RTOG in Erlangen, Germany, the 5-year OS rate is 54%; cT2-T3 is 45% and cT4 is 15% [4]. Dr. Van der Heijden states that trimodal therapy should only be considered in patients with cT2-3a tumors and is the superior bladder preservation modality.
In conclusion, Dr. Van der Heijden notes that (i) 20% of MIBC patients fit inclusion criteria for bladder preservation, (ii) trimodal therapy is the best bladder preservation modality, (iii) the keyword for success in trimodal therapy is patient selection and a radical TURBT, and (iv) shared decision making is very important with the use of decision aids.
References:
1. van der Steen-Banasik E, Ploeg M, Witjes JA, et al. Brachytherapy versus cystectomy in solitary bladder cancer: A case control, multicentre, East-Netherlands study. Radiother Oncol 2009;93(2):352-357.
2. Kulkarni GS, Hermanns T, Wei Y, et al. Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in the setting of a multidisciplinary bladder cancer clinic. J Clin Oncol 2017;35(20):2299-2305.
3. Efstathiou JA, Spiegel DY, Shipley WU, et al. Long-term outcomes of selective bladder preservation by combined-modality therapy for invasive bladder cancer: the MGH experience. Eur Urol 2012;61(4):705-711.
4. Krause FS, Walter B, Ott OJ, et al. 15-year survival rates after transurethral resection and radiochemotherapy or radiation in bladder cancer treatment. Anticancer Res 2011;31(3):985-990.
Presented by: Antoine Van Der Heijden, Radboud University Centre, Nijmegen, The Netherlands
Written by: Zachary Klaassen, MD, Urologic Oncology Fellow, University of Toronto, Princess Margaret Cancer Centre, twitter: @zklaassen_md at the 2018 European Association of Urology Meeting EAU18, 16-20 March, 2018 Copenhagen, Denmark