This study is an ongoing, prospective, randomized trial enrolling patients diagnosed with bladder cancer and undergoing endoscopic intervention. Inclusion criteria were tumor size of < 3 cm, and ≤ 3 lesions, and no sign of muscle invasion and/or ureteral involvement. The primary outcome is bladder cancer staging, and secondary outcomes include T1 substaging (microstaging systems T1a/b/c), intraoperative complications, rate of adjuvant treatment, postoperative complications, and oncologic outcomes. A total of 300 subjects will be included in the study with 1:1.5 treatment allocation for en-bloc resection of bladder tumor. From March 2018 to January 2020, 180 patients met inclusion criteria. An up to date flow diagram is as follows:
Overall, 64 (40.5%) and 94 (59.5%) patients were submitted to TURBT and en-bloc resection of bladder tumor, respectively. Pre-operatively, the populations were comparable. T1 substaging was feasible in 80% of TURBT patients versus 100% of en-bloc resection of bladder tumor patients (p=0.07). Adjuvant treatment was planned in 84% and 94% in TURBT and en-bloc resection of bladder tumor, respectively (p=0.1). The rate of obturator nerve reflex and perforation were comparable (both p=0.3), and Clavien-Dindo >2 complications were 5.3% for TURBT patients compared to 3.1% for en-bloc resection of bladder tumor. Surgical, irrigation and catheterization time were all comparable (all p>0.2). Recurrence at 3 months was 3.1% vs 2.1% in TURBT and en-bloc resection of bladder tumor (p=0.7). The complete outcomes are as follows: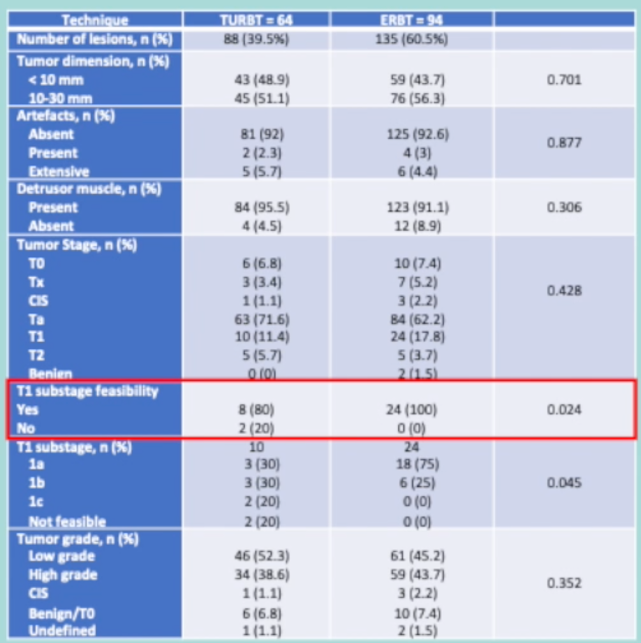
Dr. Diani concluded his presentation with the following take-home messages:
- According to the interim analysis, en-bloc resection of bladder tumor and TURBT have comparable results in terms of pathological, surgical, and oncological outcomes
- En-bloc resection of bladder tumor shows a tendency to significance in T1 substaging feasibility
- This is the first randomized study in this setting and it is warranted to define the role of en-bloc resection of bladder tumor
Presented By: Pietro Diana, MD, Department of Urology, Humanitas Clinical and Research Center, Rozzano, Italy
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
- Teoh JYC, MacLennan S, Chan VWS, et al. An International Collaborative Consensus Statement on En Bloc Resection of Bladder Tumour Incorporating Two Systematic Reviews, a Two-round Delphi Survey, and a Consensus Meeting. Eur Urol 2020 Oct;78(4):546-569.