He started by noting that cytoreductive nephrectomy is defined as the removal of the primary tumor in the presence of synchronous metastatic disease. Recent randomized trials have demonstrated similar survival among patients receiving systemic therapy alone. So the question before us is cytoreductive nephrectomy necessary? This has been an ongoing debate.
CARMENA1 and SURTIME2 have opened the debate regarding the utility of CN. Many phase 3 trials of TKI and immunotherapy showed continued survival improvement in patients who underwent CN. Multiple observational studies demonstrated a beneficial effect of CN – but are Limited by selection bias.
Based on what is published so far he feels that there is insufficient data to answer who should undergo CN, but recognizes that patient selection is probably crucial. The specific selection criteria remain to be determined.
He summarized three boxes of selection criteria, seen below:
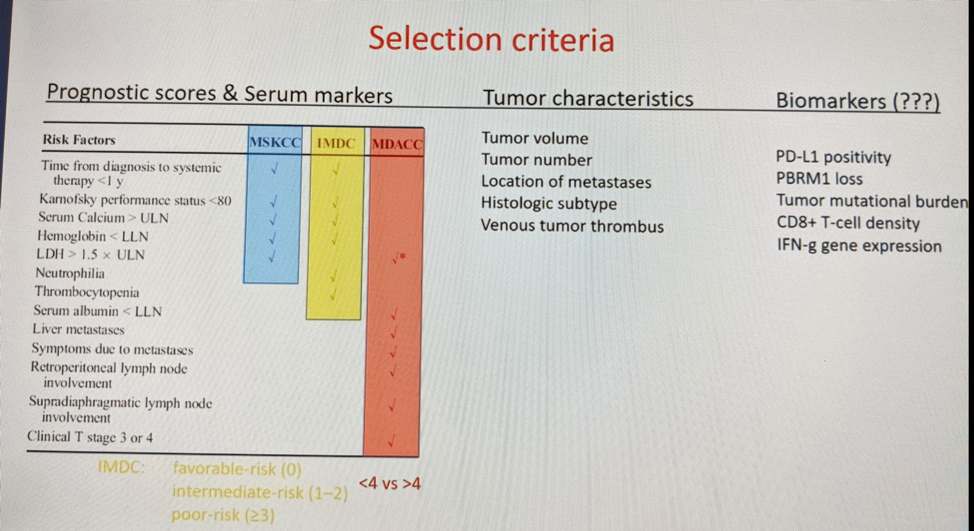
Biomarkers listed on the right are too early for clinical use. At this time prognostic scores, as seen on the left, and tumor characteristics form the basis for selection.
In this flow diagram by Shapiro et al. (The Cancer Journal 2020), a modern selection criteria is delineated. He agrees with the selection criteria listed.

At this point patients that are most likely to benefit have only one of the following:
- <= metastases other than adrenal or pulmonary (low volume oligometastatic)
- Significant systemic symptoms
- Serum derangement
Generally, this includes patients with good PS (who can undergo surgery), limited metastatic burden, symptomatic primary tumor, or MDACC low-risk/IMDC favorable/intermediate risk.
Presented by: George N. Thalmann, University of Bern, Switzerland
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Assistant Professor of Urology, Sidney Kimmel Cancer Center, Thomas Jefferson University, @tchandra_uromd on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
- Méjean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma. New England Journal of Medicine 2018;379:417-27.
- Bex A, Mulders P, Jewett M, Wagstaff J, van Thienen JV, Blank CU, van Velthoven R, Del Pilar Laguna M, Wood L, van Melick HHE, Aarts MJ, Lattouf JB, Powles T, de Jong Md PhD IJ, Rottey S, Tombal B, Marreaud S, Collette S, Collette L, Haanen J. Comparison of Immediate vs Deferred Cytoreductive Nephrectomy in Patients With Synchronous Metastatic Renal Cell Carcinoma Receiving Sunitinib: The SURTIME Randomized Clinical Trial. JAMA Oncol. 2019 Feb 1;5(2):164-170. doi: 10.1001/jamaoncol.2018.5543. Erratum in: JAMA Oncol. 2019 Feb 1;5(2):271. PMID: 30543350; PMCID: PMC6439568.