(UroToday.com) The joint session of the European Association of Urology EAU and the Confederacion Americana de Urologia included a session discussing the surgical treatment of lymph node recurrences after radical prostatectomy. Dr. Nicola Fossati from San Raffaele, Milan took the pro surgery approach for his presentation.
Dr. Fossati’s first point is that regarding salvage lymph node dissection there is a discrepancy between clinical practice and level of evidence. There have been 102 articles published on salvage lymph node dissection, however, the majority are retrospective studies with a low level of evidence. Thus, the 2021 EAU guidelines do not have recommendations regarding salvage lymph node dissection indications nor patient selection.
Secondly, when considering salvage lymph node dissection, patient selection is essential. Previous work from Dr. Fossati’s group has sought to identify the optimal candidates for salvage lymph node dissection based on preoperative characteristics.1 In this study, 654 patients who experienced PSA rise and nodal recurrence after radical prostatectomy underwent salvage lymph node dissection, where lymph node recurrence was documented by PET/CT scan using either 11C-choline or 68Ga-labeled PSMA ligand. The primary outcome was early clinical recurrence within 1 year of salvage lymph node dissection. Over a median follow-up of 30 (IQR 16-50) months, 334 patients developed clinical recurrence after salvage lymph node dissection. There was a 30% clinical recurrence rate at 1 year, and a 50% clinical recurrence rate at 3 years. Overall, 20% of patients were free from hormonal therapy and biochemical recurrence at 3 years:
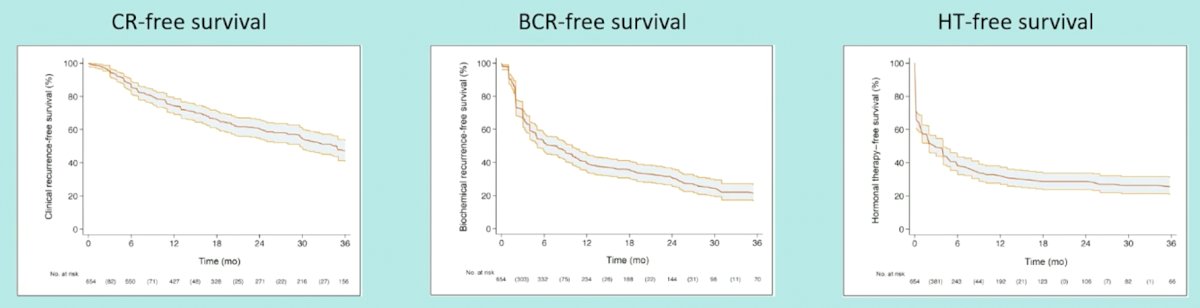
Using multivariable analysis, Gleason grade group 5 (HR 2.04; p<0.0001), time from radical prostatectomy to PSA rising (HR 0.99; p=0.025), hormonal therapy administration at PSA rising after radical prostatectomy (HR 1.47; p=0.0005), retroperitoneal uptake at PET/CT scan (HR 1.24; p=0.038), three or more positive spots at PET/CT scan (HR 1.26; p=0.019), and PSA level at salvage lymph node dissection (HR: 1.05; p<0.0001) were significant predictors of clinical recurrence after salvage lymph node dissection.
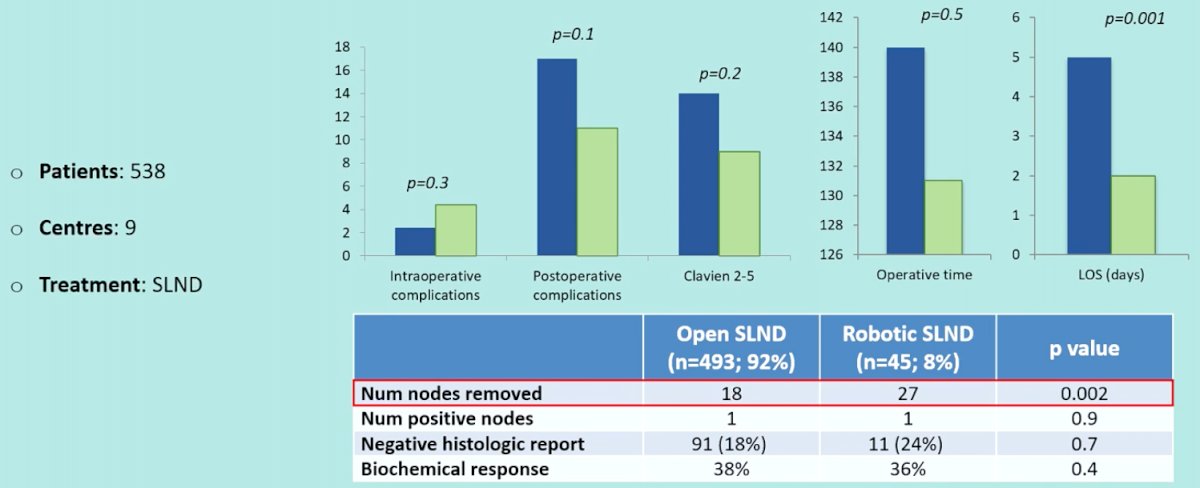
Dr. Fossati’s third point is that surgical morbidity is changing. With the advent of minimally invasive approaches, morbidity has decreased substantially. Patients undergoing robotic salvage lymph node dissection have less blood loss, shorter length of stay, and fewer 30-day complications. Highlighting data presented at the EAU 2017 annual meeting, Dr. Fossati notes that a robotic salvage lymph node dissection was associated with a median of 27 lymph nodes removed compared to 18 for the open approach (p=0.002):
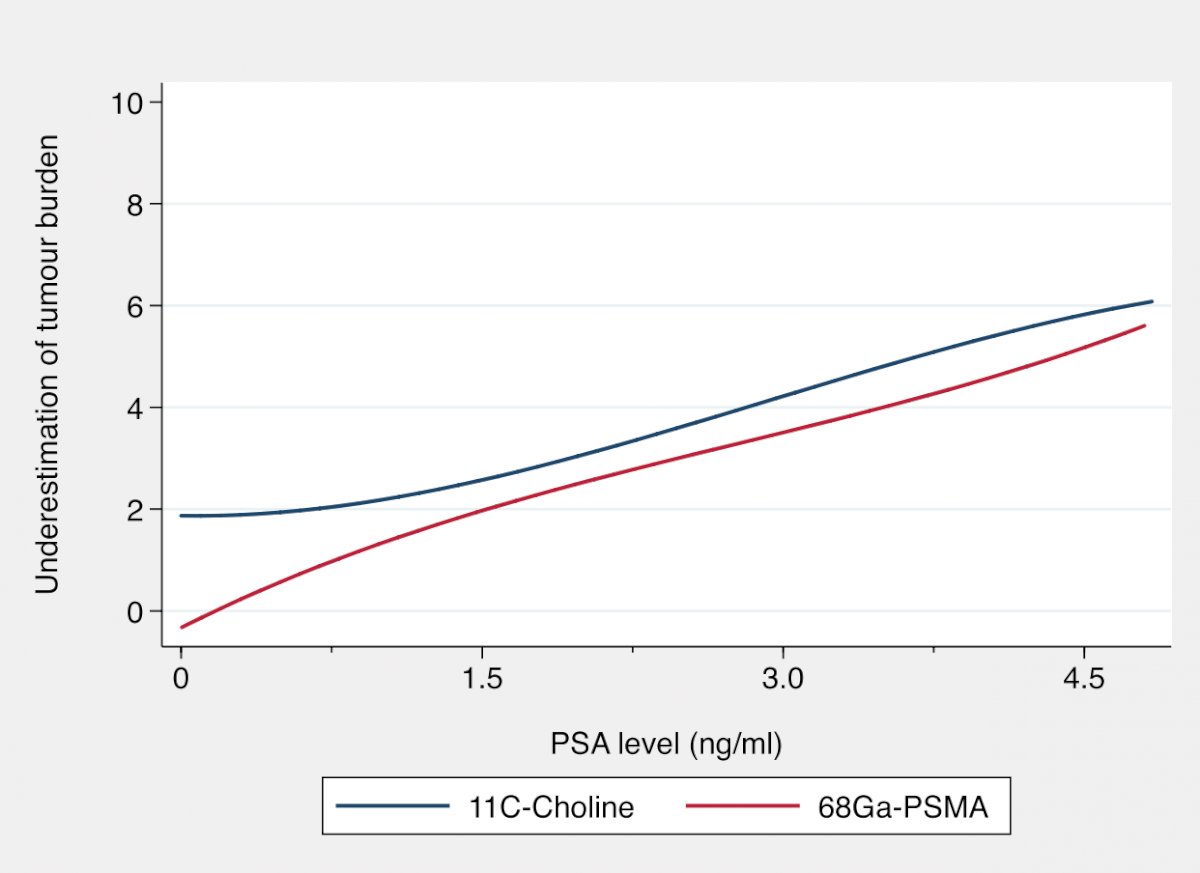
Fourthly, Dr. Fossati highlights that imaging underestimates the tumor burden for these patients. Dr. Fossati’s group has compared the use of 11C-choline and 68Ga-PSMA in men undergoing salvage lymph node dissection for nodal recurrent prostate cancer. Among 641 patients, lymph node recurrence was documented by PET/CT using 11C-choline (407, 63%) or 68Ga-PSMA ligand (234, 37%). Overall, the extent of tumor burden underestimation was significantly higher in the 11C-choline group compared to the 68Ga-PSMA group (p <0.0001), which was confirmed on multivariable analysis (p=0.028). Outcomes stratified by imaging modality at various PSA level are as follows:
Finally, histology and genomic information are available after salvage lymph node dissection. This information may have prognostic value, allows targeting of systemic therapy (ie. olaparib for HRR mutations), and provides tissue for biobanks for future research.
To summarize his talk, Dr. Fossati re-emphasized the five key points for consideration of salvage lymph node dissection:
- There is low level of evidence
- Patient selection is essential
- Surgical morbidity is changing
- Imaging underestimates tumor burden
- Histology and genomic information is available after salvage lymph node dissection
Presented by: Nicola Fossati, Urological Research Institute, IRCCS Ospedale San Raffaele, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
- Fossati N, Suardi N, Gandaglia G, et al. Identifying the optimal candidate for salvage lymph node dissection for nodal recurrence of prostate cancer: Results from a large, multi-institutional analysis. Eur Urol. 2019 Jan;75(1):176-183.
- Fossati N, Scarcella S, Gandaglia G, et al. Underestimation of positron emission tomography/computerized tomography in assessing tumor burden in prostate cancer nodal recurrence: Head-to-head comparison of 68Ga-PSMA and 11C-choline in a large, multi-institutional series of extended salvage lymph node dissection. J Urol. 2020 Aug;204(2):296-302.