He starts by reviewing the literature. He begins with a study by Coen et al.1, a retrospective study of 1498 men with median follow-up 70 months, in which they evaluate the impact of persistent local tumor on metastases-free survival. As seen below, in patients in which the primary tumor was not treated, there was a much higher late of recurrent metastatic disease.
They concluded that local tumor persistence was associated with a late wave of metastases. This hinted at the need for local control.
Ventimiglia et al. completed a systematic review of 5 observational studies assessing the impact of local therapy on node positive prostate cancer. One study (Seisen et al.2) allowed for RP or XRT to the primary, while the remaining four only allowed for XRT. Lin et al.3 looked at EBRT for cN+ disease patients using the National Cancer Database in a propensity matched analysis – this was a retrospective study. They found that XRT addition was associated with a 50% mortality reduction. Seisen et al.2 also utilized the NCDB but expanded to include patients undergoing RP with or without ADT.
Any local therapy was associated with significant survival benefit – and there was no significant difference between RT or RP (as seen below).
Some unanswered questions:
1. While pelvic RT ~54 Gy is sufficient for microscopic disease, may not be sufficient for macroscopic disease
2. What is the role of PSMA/PET CT or MRI?
3. Goal of RT-boost to all positive nodes (curative dose)?
4. For RP – aim should be to remove all macroscopic positive nodes.
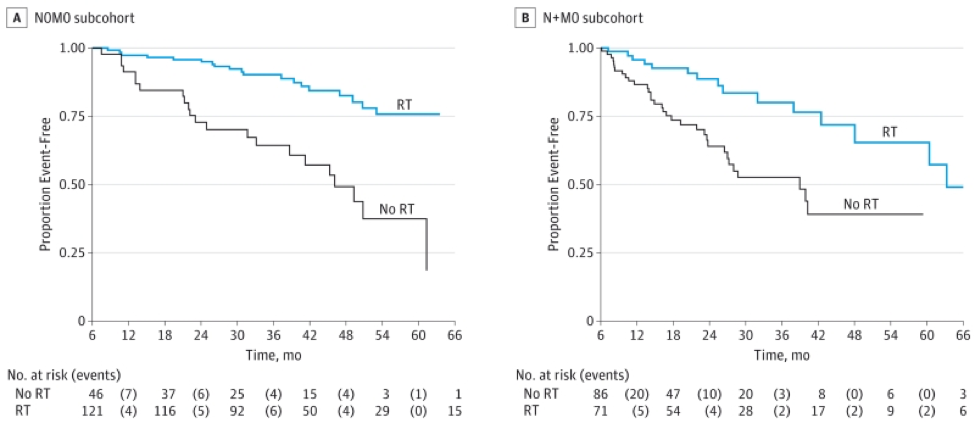
He highlighted some of the STAMPEDE data4 to indicate that there is strong RCT data to support that XRT in this setting is working. This is seen in the KM curve on the right:
He concludes with the guideline statement from the EAU:
Offer patients with cN1 disease a local treatment (either RP or IMRT plus image-guided radiotherapy) plus long-term ADT. This is a weak recommendation.
Presented by: Thomas Wiegel, MD, PhD, Professor, Medical Director, Deaprtment of Radiation Therapy and Radiation Oncology, Ulm University Hospital
References:
1. Coen JJ, Zietman AL, Thakral H, et al. Radical radiation for localized prostate cancer: local persistence of disease results in a late wave of metastases. J Clin Oncol. 2002 Aug 1;20(15):3199-205. doi: 10.1200/JCO.2002.01.086. PMID: 12149291.
2. Ventimiglia E, Seisen T, Abdollah F,et al. A Systematic Review of the Role of Definitive Local Treatment in Patients with Clinically Lymph Node-positive Prostate Cancer. Eur Urol Oncol. 2019 May;2(3):294-301. doi: 10.1016/j.euo.2019.02.001. Epub 2019 Mar 23. PMID: 31200844.
3. Seisen T, Vetterlein MW, Karabon P, et al. Efficacy of Local Treatment in Prostate Cancer Patients with Clinically Pelvic Lymph Node-positive Disease at Initial Diagnosis. Eur Urol. 2018 Mar;73(3):452-461. doi: 10.1016/j.eururo.2017.08.011. Epub 2017 Sep 8. PMID: 28890245.
4. 1. Parker CC, James ND, Brawley CD, et al; Systemic Therapy for Advanced or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investigators. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018 Dec 1;392(10162):2353-2366. doi: 10.1016/S0140-6736(18)32486-3. Epub 2018 Oct 21. PMID: 30355464; PMCID: PMC6269599.