(UroToday.com) The 2024 European Association of Urology (EAU) annual congress held in Paris, France between April 5th and 8th was host to a non-muscle invasive bladder cancer (NMIBC) poster session of studies evaluating the benefits and harms of various treatment options. Dr. Kevin Gallagher presented the results of the RESECT cluster randomized trial which evaluated whether audit, feedback, and education can improve quality indicator metrics and reduce early recurrence rates with transurethral resection of bladder tumor (TURBT) for NMIBC.
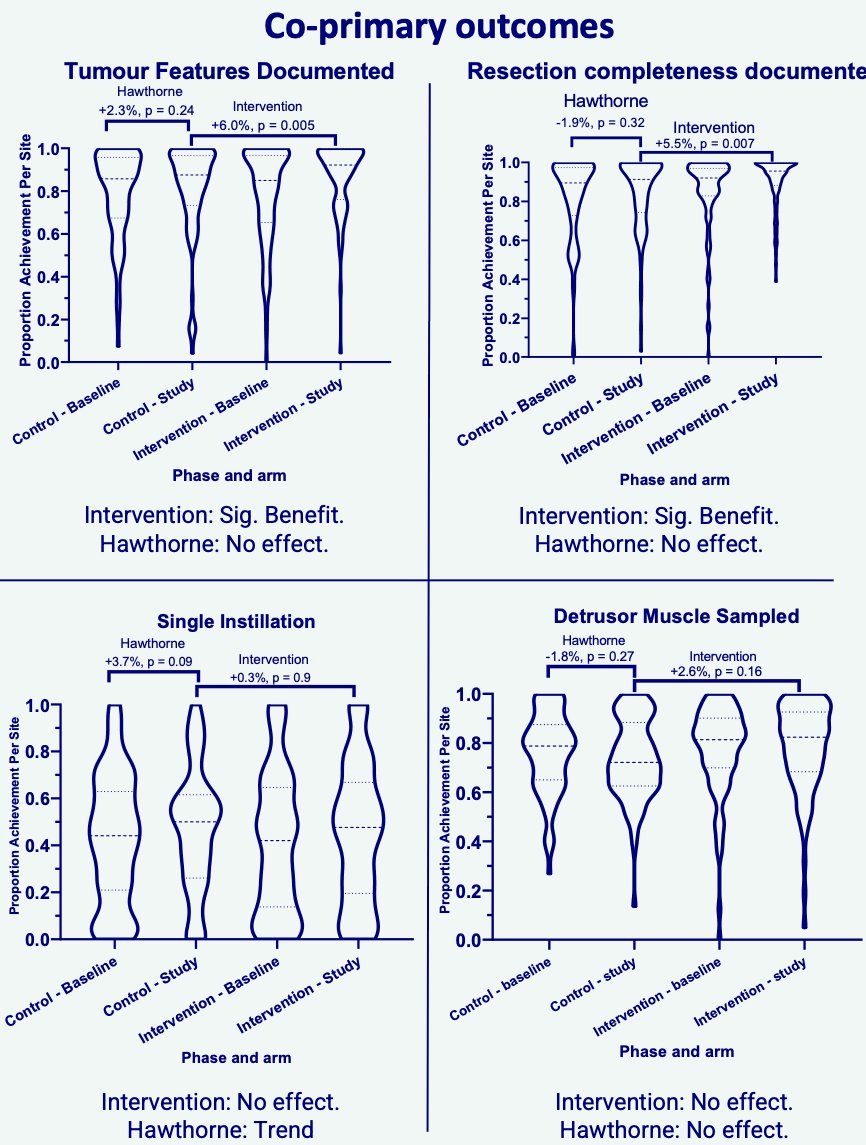
This was an international, multicenter observational study, with an embedded cluster randomised trial, of an institution-targeted web-based performance feedback and educational tool (intervention group) versus standard of care (no performance feedback; control group). There were four co-primary outcomes, each adjusted for baseline achievement:
- Detrusor muscle sampling
- Single instillation intravesical chemotherapy administration
- Resection completeness documentation
- Key tumor feature documentation
The recurrence rate at the first cystoscopy following complete TURBT was a secondary endpoint, assessed at the patient level following adjustment for surgeon, site (random effects), and tumour number, size, grade, and stage (fixed effects). Participating sites were excluded if they did not submit data for at least 20 eligible cases in both phases.
This study included 201 sites that recruited 15,879 patients between October 2021 and March 2023. Of these 201 sites, 100 were ‘intervention’ sites and 101 were ‘control’ sites. The arms were comparable for patient, tumor, and site level variables.
‘Intervention’ sites with feedback and education tools had significantly improved achievement of resection completeness and key tumor feature documentation, with adjusted mean differences of 5.6% (p=0.006) and 6.1% (p=0.005), respectively. There were no significant differences in the rates of single instillation intravesical chemotherapy administration, detrusor muscle sampling, or early recurrences.
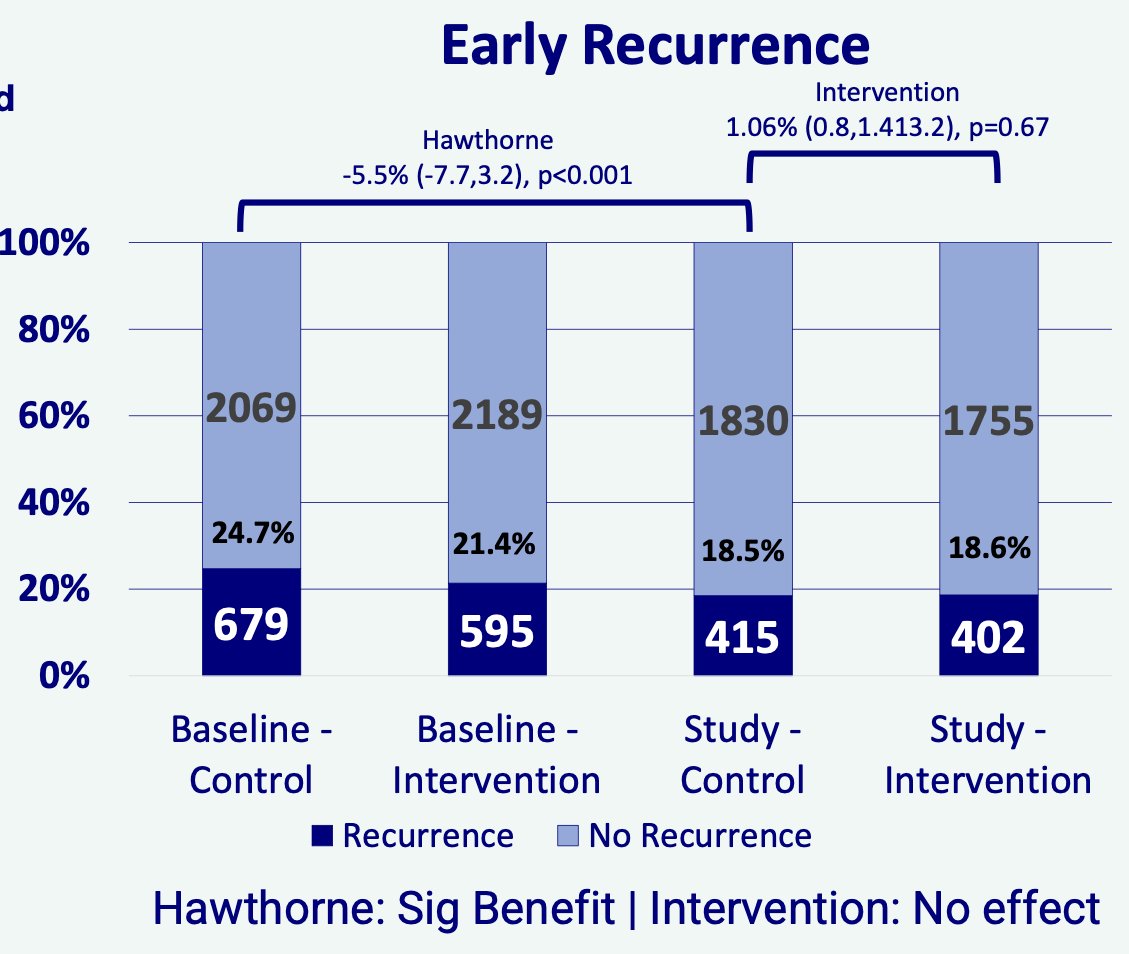
Of note, in the control arm, the early recurrence rate was significantly lower in the prospective phase (18.5%) compared to the retrospective phase (24.7%) after adjusting for tumour size, number, grade, and stage (adjusted difference: -5.5%, p<0.001).
Dr. Gallagher and colleagues concluded that web-based feedback and education intervention can improve some quality performance indicators but not early recurrence rates following TURBT. There is a Hawthorne effect in TURBT surgery – “being watched” appears to have resulted in improvements in practice and outcomes. This study suggests that multicenter TURBT audit with feedback is likely to improve quality and outcomes in TURBT surgery.
Presented by: Kevin Gallagher, MBChB, PhD, Specialist Trainee in Urological Surgery, Fellow for Data Driven Innovation, Clinical Lecturer, The University of Edinburgh, Edinburgh, Scotland
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 European Association of Urology (EAU) annual congress, Paris, France, April 5th – April 8th, 2024