The 2024 European Association of Urology (EAU) annual meeting featured a session on navigating urothelial carcinoma from innovative diagnostics to therapeutic strategies, and a presentation by Dr. Jose Subiela discussing a potential role for BCG in very high-risk non-muscle invasive bladder carcinoma.
The EAU updated non-muscle invasive bladder carcinoma risk stratification in 2021, establishing a criterion for the new “very high risk” group, defined as patients with at least a 20% chance of disease progression over 5 years. This identified a group with a 5-year progression risk of 44%. Consequently, current guidelines suggest upfront radical cystectomy for all very high-risk non-muscle invasive bladder carcinoma. However, excluding patients who have undergone BCG therapy from this risk group raises concerns about potential overtreatment. The aim of this study presented at EAU 2024 was to assess the oncological outcomes in very high-risk non-muscle invasive bladder carcinoma patients who have received adequate BCG therapy.
This study was a multi-institutional retrospective study involving patients with very high-risk non-muscle invasive bladder carcinoma (according to EAU risk stratification) who received adequate BCG therapy from 2007 to 2020 (n = 640). Patients were categorized by BCG maintenance duration (<1 year, >1-2 years, >2 years). Kaplan-Meier analysis estimated recurrence-free survival, progression-free survival, cancer-specific survival, and overall survival. Conditional survival probabilities for 0-4 years without events were computed, and Cox regression assessed predictors of oncological outcomes. The Aalen Johansen method was used to assess the cumulative incidence for overall mortality and cancer specific mortality after accounting for other causes of mortality as competing risks.
A total of 640 patients were included, with 405 receiving <1-year, 169 receiving ≥1-2-years, and 66 receiving >2-years of BCG maintenance. The baseline characteristics for the overall cohort is as follows: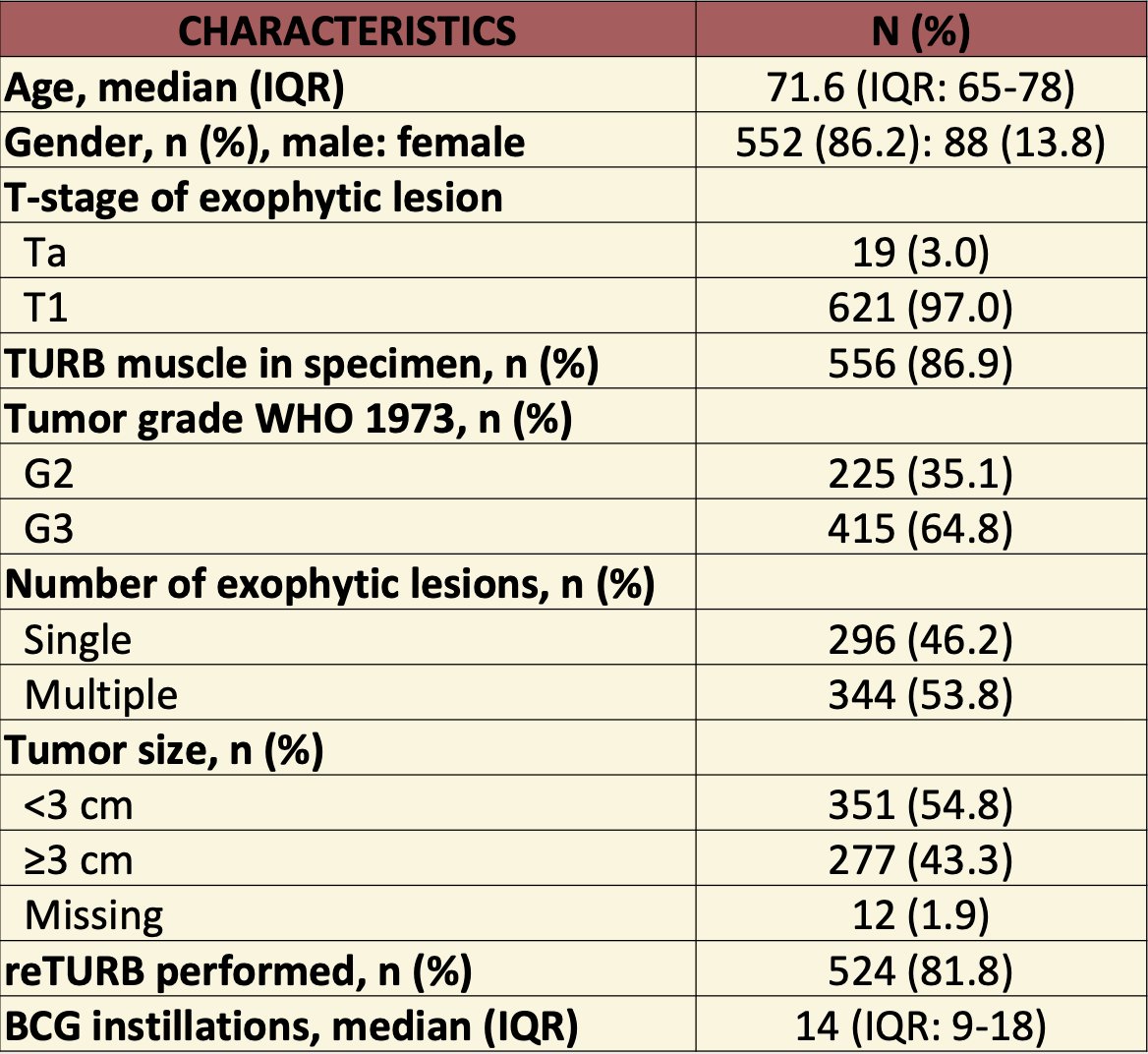
The median follow-up was 47 months follow-up (95% CI 32-67) for those event-free. The 5-year rates for recurrence-free survival, high-grade recurrence-free survival, progression-free survival, overall survival, and cancer-specific survival were as follows: 48% (95% CI 44-52), 78% (95% CI 74-82), 71% (95% CI 67-75), and 86% (95% CI 82-90), respectively: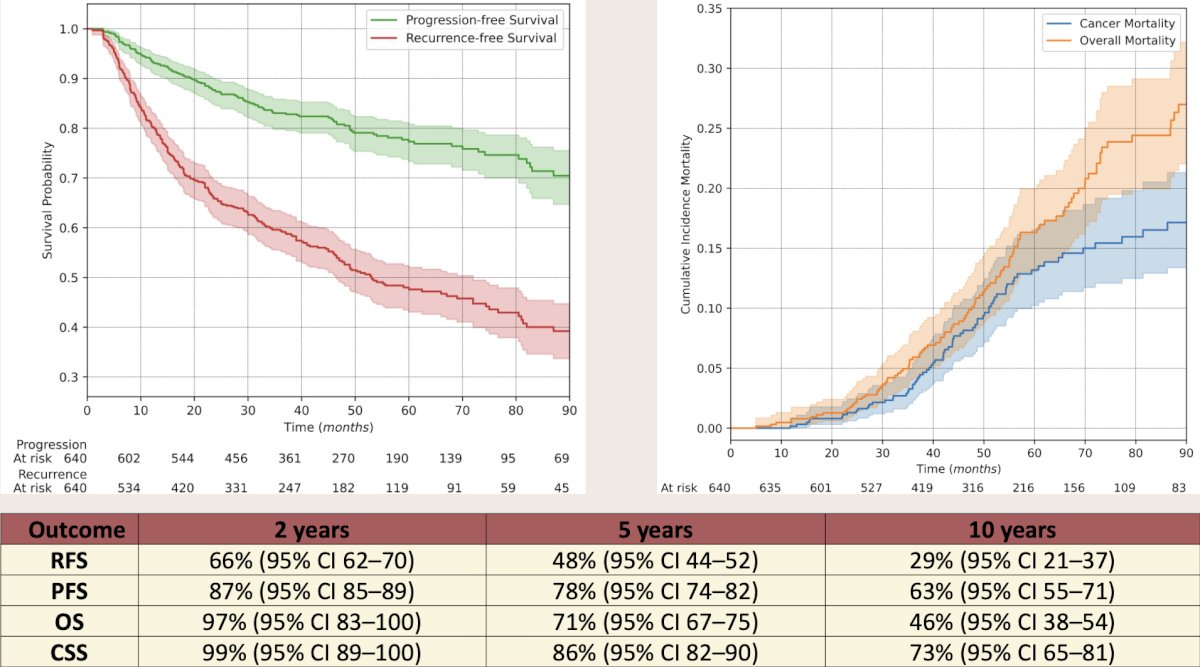
The survival analysis revealed that the ≥1-2-year and >2-year treatment groups showed superior outcomes compared to the <1-year group in all analyses, with no significant differences between the ≥1-2-year and >2-year groups. Multivariate Cox regression confirmed that a longer BCG treatment significantly improved outcomes. The flexible proportional model shows that in the patients receiving <1 year of BCG treatment both recurrence and progression initially rise, peaking around one year post-diagnosis suggesting that the benefit of the BCG diminishes after treatment discontinuation. Importantly, this risk peak is notably absent in those receiving longer BCG treatment (≥ 1 year). The 5-year conditional recurrence-free survival, progression-free survival, overall survival, and cancer-specific survival at 0-4 years (corresponding to 5 and 9 years from diagnosis) were: 48-91%, 78-96%, 71-87%, and 86-94%.
Dr. Subiela concluded his presentation discussing a potential role for BCG in very high-risk non-muscle invasive bladder carcinoma with the following statements:
- The patients with very high-risk non-muscle invasive bladder carcinoma who receive adequate BCG therapy experience a more favorable prognosis than that forecasted by the EAU risk groups, particularly in long-term adherents (at least 2 years)
- Although this study is not advocating for BCG as first-line therapy in all cases, a case-specific approach is essential for decision-making
- The prognosis of patients with very high-risk non-muscle invasive bladder carcinoma improves over time
- As a result, the probability of recurrence and progression is sufficiently low when patients remain disease-free for four years to justify less strict follow-up
Presented by: Jose D. Subiela, MD, Hospital Universitario Ramón y Cajal, Madrid, Spain
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, WellStar MCG Health, @zklaassen_md on Twitter during the 2024 European Association of Urology (EAU) annual congress, Paris, France, April 5th - April 8th, 2024