(UroToday.com) The 2024 European Association of Urology (EAU) annual meeting featured a plenary session on living with advanced kidney cancer and urothelial cancer, and a state of the art lecture presentation by Dr. Shankar Siva discussing advancements in cutting-edge stereotactic ablative radiation therapy for oligometastatic kidney cancer. Dr. Siva notes that the classical teaching is that RCC is radioresistant.
However, stereotactic ablative radiation therapy has been used in metastatic RCC for years. In a meta-analysis of 28 studies, Zaorsky et al. assessed 1,602 mutually exclusive patients (679 extracranial/923 intracranial lesion) and 3,892 total lesions (1,159 extracranial/2,733 intracranial).1 Overall, the 1-year intracranial local control rate was 90.1% and was 89.1% for 1-year extracranial local control: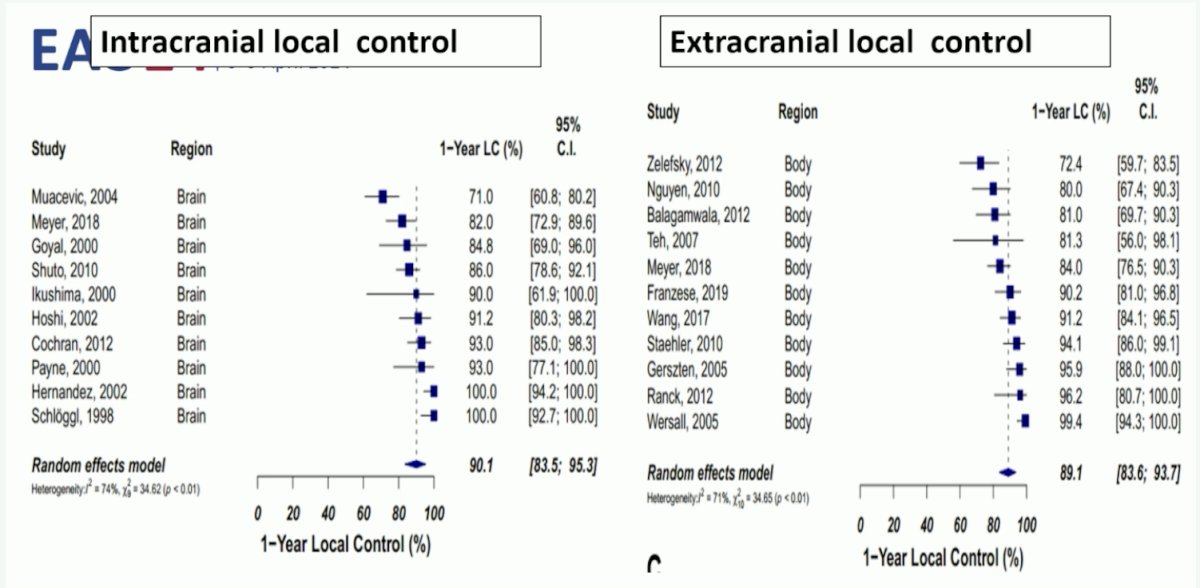
What we know from prospective clinical trials of stereotactic ablative radiation therapy in oligometastatic RCC is that this modality has been investigated in three scenarios:
- In lieu of systemic therapy
- Combined with immunotherapy
- To delay next line of systemic therapy in ‘oligoprogressive’ disease
The RAPPORT trial is a phase 1/2 trial of 30 patients that used stereotactic body radiotherapy to all metastases followed by 6 months of pembrolizumab.2 The concept of this trial is synergy through immunotherapy, inducing tumor antigen release into the tumor microenvironment, and with cytokine release priming the tumor microenvironment and allowing homing of cytotoxic T-cells. This transforms a “cold” microenvironment to “hot”. In RAPPORT, the median number of metastases was 3 (for n = 30, 83 metastatic sites, a larger burden than usual), with a median PFS of 15.6 months, and median overall survival and duration of response not reached. The combination was locally effective, with a 2-year local control rate of 92%: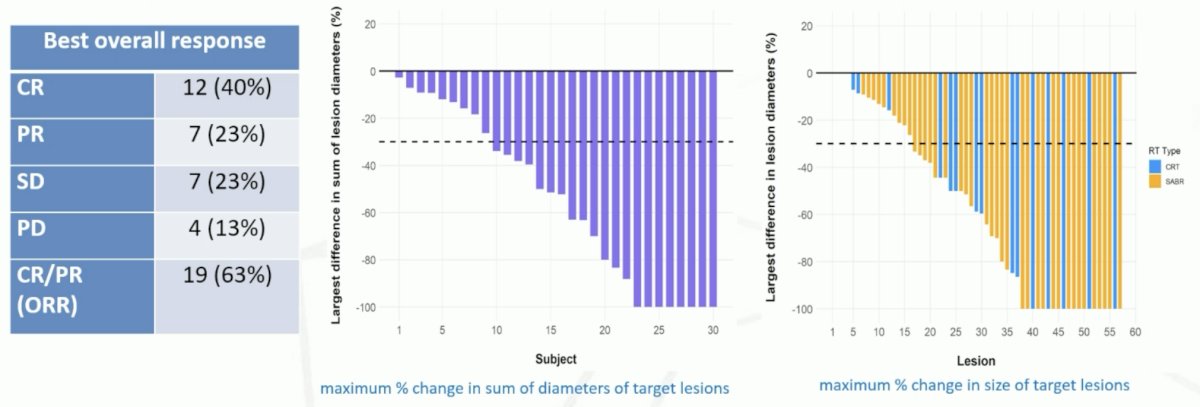
A second trial assessing stereotactic ablative radiation therapy (without systemic therapy) in low volume, oligometastatic, favorable risk patients, showed comparable results to the RAPPORT trial of higher volume patients with the addition of pembrolizumab:3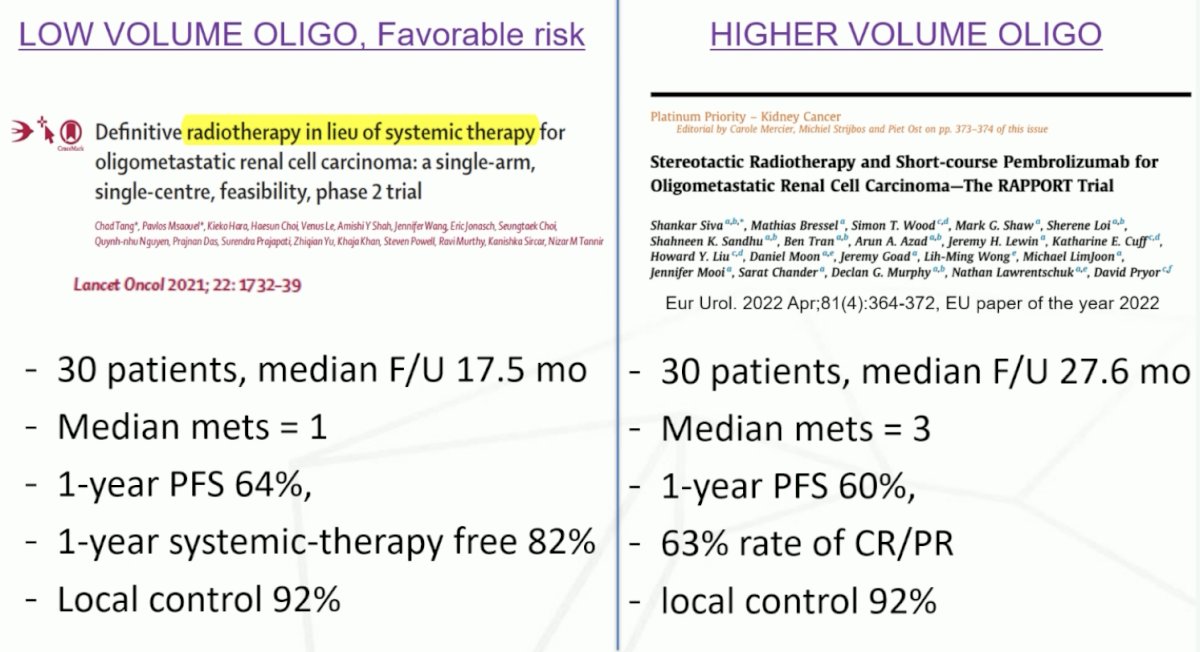
Stereotactic ablative radiation therapy has also been assessed in combination with TKIs for oligoprogressive disease. In a phase 2 trial by Cheung et al., 37 patients with 1-3 “oligoprogressive” metastases were treated, noting a 1-year local control rate of 93%, median PFS after radiotherapy of 9.3 months, median time to drug therapy switch of 12.6 months, and no grade 3-5 toxicities.4 A second phase 2 trial by Hannan et al. assessed 20 patients with 1-3 “oligoprogressive” metastases that were treated, noting a 1-year local control rate of 100%, median time to drug therapy switch of 11.1 months, with one grade toxicity, and no grade 4-5 toxicities.5
Dr. Siva notes that the NCCN guidelines support stereotactic ablative radiation therapy for both clear cell and non-clear cell histology, in line with surgical metastasectomy, when appropriate. Moreover, this is also supported in the ASCO guidelines. There are several advantages for both stereotactic ablative radiation therapy and surgery:
- Stereotactic ablative radiation therapy: non-invasive, low toxicity that does not interrupt drug therapy, and synergy with immunotherapy
- Surgery: tissue confirmation and rapid palliation of the mass effective (ie. for neurologic symptoms)
Dr. Siva concluded his presentation discussing advancements in cutting-edge stereotactic ablative radiation therapy for oligometastatic kidney cancer by summarizing what we know from prospective trials in oligometastatic RCC:
- For surgery, the addition of a TKI is not beneficial:
- RESORT trial of sorafenib versus metastasectomy alone6
- ECOG-ACRIN 2810 of pazopanib versus placebo (Appleman et al, JCO 2019 abstract)
- Stereotactic ablative radiation therapy can:
- Be delivered in lieu of systemic therapy3
- Delay next line of systemic therapy in oligoprogressive disease4-5
- Be safe and effective when combined with a short course of immunotherapy2
There are several future directions that Dr. Siva highlighted, including the NRG SAMURAI phase III trial randomizing mRCC patients to standard immunotherapy versus stereotactic ablative radiation therapy to the primary (42 Gy in 3 fractions) + standard immunotherapy: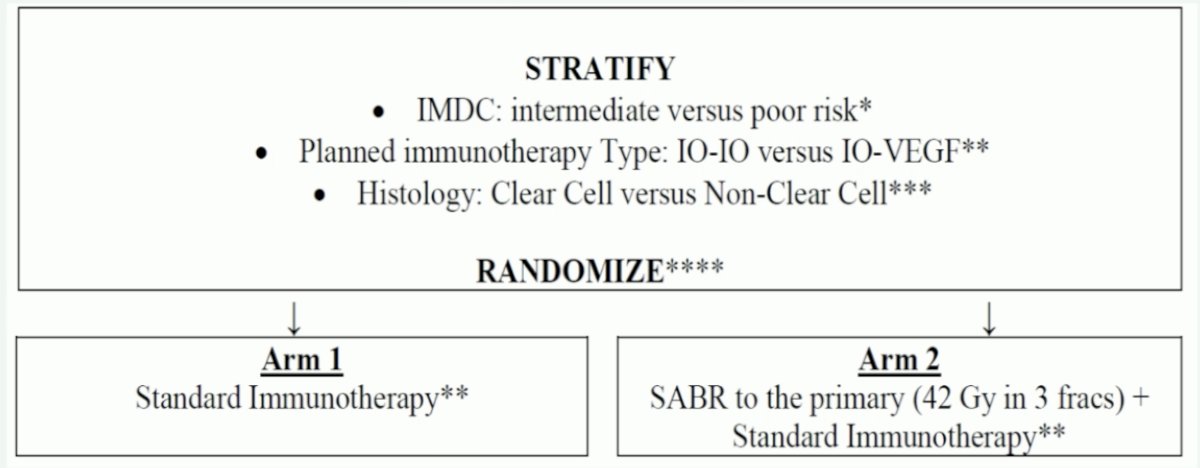
Additionally, there is the potential for screening with PSMA PET imaging and treating metastases with stereotactic ablative radiation therapy, followed by assessment of treatment response with subsequent PSMA PET imaging: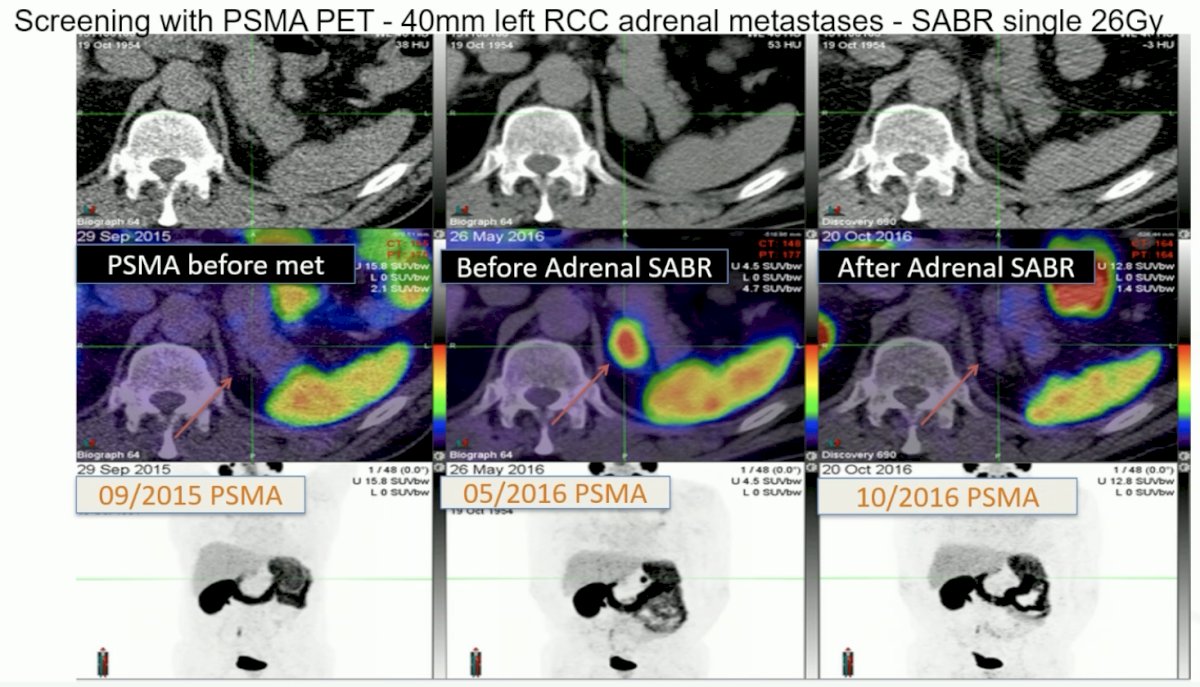
Presented by: Shankar Siva, Peter MacCallum Cancer Centre, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, WellStar MCG Health, @zklaassen_md on Twitter during the 2024 European Association of Urology (EAU) annual congress, Paris, France, April 5th - April 8th, 2024
References:
- Zaorsky NG, Lehrer EJ, Kothari G, et al. Stereotactic ablative radiation therapy for oligometastatic renal cell carcinoma (SABR ORCA): A meta-analysis of 28 studies. Eur Urol Oncol. 2019 Sep;2(5):515-523.
- Siva S, Bressel M, Wood ST, et al. Stereotactic Radiotherapy and Short-course Pembrolizumab for Oligometastatic Renal Cell Carcinoma—The RAPPORT Trial. Eur Urol. 2022;81(4):364-472.
- Tang C, Msaouel P, Hara K, et al. Definitive radiotherapy in lieu of systemic therapy for oligometastatic renal cell carcinoma: A Single-arm, single-centre, feasibility, phase 2 trial. Lancet Oncol. 2021;22:1732-1739.
- Cheung P, Patel S, North SA, et al. Sereotactic radiotherapy for Oligoprogression in Metastatic Renal Cell Cancer Patients Receiving Tyrosine Kinase Inhibitor Therapy: A Phase 2 Prospective Multicenter Study. Eur Urol 2021 Dec;80(6):693-700.
- Hannan R, et al. Phase II Trial of Stereotactic Ablative Radiation for Oligoprogressive Metastatic Kidney Cancer. Eur Urol Oncol. 2022 Apr;5(2):216-224.
- Procopio G, Apollonio G, Cognetti F, et al. Sorafenib versus observation following radical metastasectomy for clear cell renal cell carcinoma: Results from the phase 2 randomized open-label RESORT study. Eur Urol Oncol. 2019 Nov;2(6):699-707.