(UroToday.com) The 2024 European Association of Urology (EAU) annual meeting featured a kidney cancer rapid fire debate, and a presentation by Dr. Axel Bex discussing that delayed cytoreductive nephrectomy (dCN) plays a role in intermediate risk metastatic RCC.
For context, the case based on this discussion was a 62 year old male with a 50-year smoking history, with a history of hepatitis C (in remission), DVT in 2000, and COPD with NYHA 1 dyspnea. Otherwise, he had an excellent performance status. Given his dyspnea, he received a CT of the chest which revealed several ~1 cm pulmonary nodules, which prompted a CT of the abdomen demonstrating a large 11 cm left renal mass. His lab work was normal (including creatinine) and his physical examination was otherwise normal. Thus, he was categorized as IMDC criteria intermediate risk given delay between diagnosis and systemic therapy initiation of < 12 months. He ultimately underwent a kidney biopsy that demonstrated clear cell RCC, ISUP grade 3.
Dr. Bex started his discussion arguing for delayed nephrectomy by challenging whether this patient really is intermediate risk disease: do we really know that he requires systemic therapy within a year? There are studies suggesting observation after cytoreductive nephrectomy is safe, with a time to progression of 6 months and median time to targeted therapy of 16 months. Shorter time to treatment in these patients is associated with higher IMDC risk group and higher Fuhrman grade of disease. So, whether he is truly intermediate risk disease matters in the algorithm for consideration of cytoreductive nephrectomy versus immune checkpoint inhibitor combination therapy: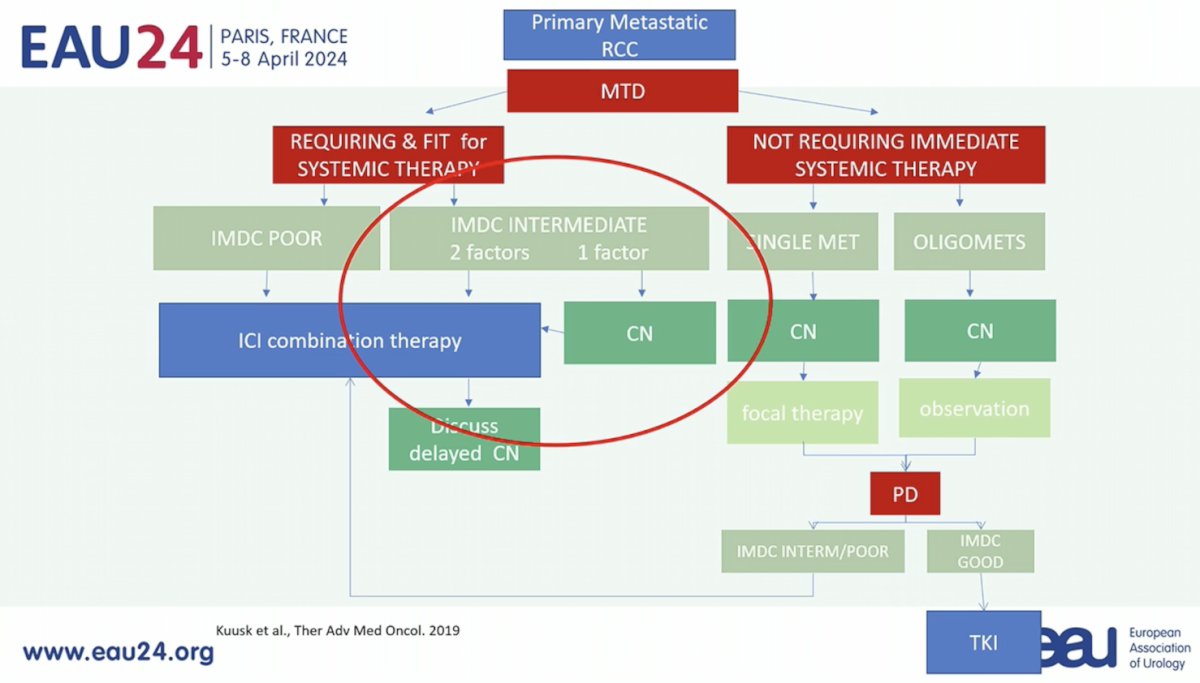
Dr. Bex notes that the pattern and dynamics of RCC metastases are quite heterogeneous and may be due to “punctuated evolution” ie. rapid progression or “branched evolution” ie. attenuated progression:
Assessing the overall survival data in CARMENA1 and SURTIME,2 it is important to note that overall survival was the primary endpoint in CARMENA with no difference in survival outcome between nephrectomy followed by sunitinib versus sunitinib alone (HR 0.97, 95% CI 0.79-1.19). However, 43% of patients in CARMENA were MSKCC poor risk disease. In SURTIME, overall survival was a secondary endpoint, and there was an improvement in survival with delayed cytoreductive nephrectomy versus immediate nephrectomy (HR 0.57, 95% CI 0.34-0.95), with only 11% of patients having MSKCC poor risk disease: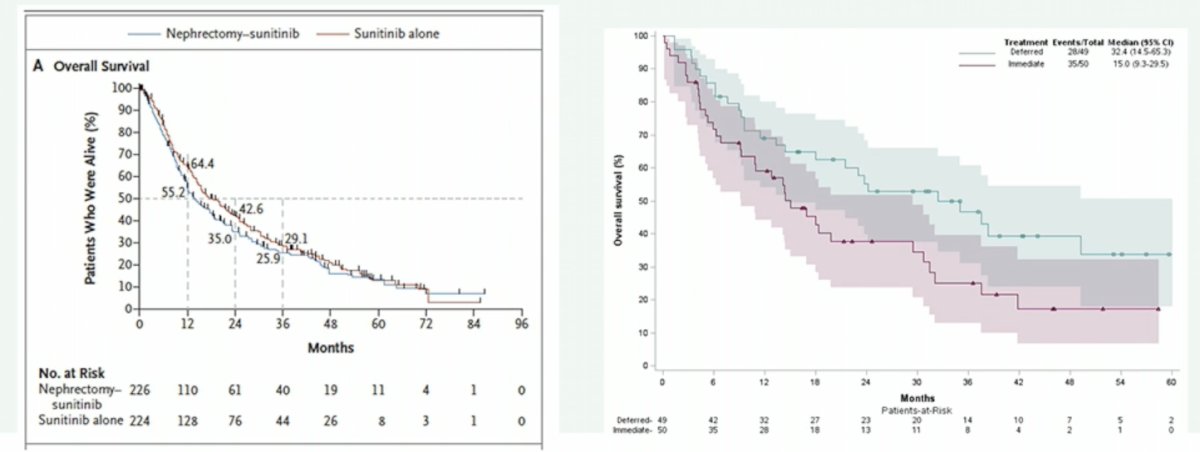
Thus, this patient better fits SURTIME criteria and the potential benefit of delayed cytoreductive nephrectomy. Dr. Bex highlighted that in the metastatic RCC immune checkpoint inhibitor trials, those patients treated with the primary tumor in place generally had improved progression free and overall survival, compared to sunitinib alone:
Thus, the EAU RCC 2021 guidelines state that “patients with their primary tumor in place treated with immune checkpoint inhibitor-based combination therapy have better PFS and OS in exploratory subgroup analyses compared to treatment with sunitinib” Category 2b recommendation.
To conclude his presentation, Dr. Bex highlighted work presented earlier at EAU 2024 from a Dutch-UK database of which there was a cohort of patients treated with their primary tumor in place and received nivolumab + ipilimumab combination therapy. Among all 177 patients (those receiving and not receiving surgery), the IMDC intermediate risk patients had a median overall survival of 49.8 months:
Specifically looking at the 30 patients (17%) that underwent deferred cytoreductive nephrectomy after a median preoperative duration of nivolumab + ipilimumab of 14.5 months, these patients performed much better than those that did not undergo delayed cytoreductive nephrectomy:
Presented by: Axel Bex, MD, PhD, Royal Free Hospital, London, UK
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, WellStar MCG Health, @zklaassen_md on Twitter during the 2024 European Association of Urology (EAU) annual congress, Paris, France, April 5th - April 8th, 2024
References:
- Mejean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal cell carcinoma. N Engl J Med 2018 Aug 2;379(5):417-427.
- Bex A, Mulders P, Jewett M, et al. Comparison of immediate vs deferred cytoreductive nephrectomy in patients with synchronous metastatic renal cell carcinoma receiving sunitinib: The SURTIME Randomized Clinical Trial. JAMA Oncol 2019 Feb 1;5(2):164-170.