(UroToday.com) The 2024 European Association of Urology (EAU) annual meeting featured a plenary session on living with advanced kidney cancer and urothelial cancer, and a presentation by Dr. Sarah Psutka discussing that for first line metastatic kidney cancer less is more.
Dr. Psutka notes that the question at hand is: “Should intensified systemic therapy with triplet combinations be the new standard of care for first-line treatment of metastatic renal cell carcinoma?” There are several requirements to accept treatment intensification as the new standard:
- Improved efficacy
- Reduced (or similar) harms
- Negligible impact on future treatment, eligibility, and efficacy
Ultimately, the goal in cancer therapy is for a cure, specifically durable eradication of disease. But, Dr. Psutka notes that it is more complicated than that. Based on a 2022 survey of kidney cancer survivors, when asked “When thinking about therapy for metastatic cancer, what is the most important desire or outcome you want to see from treatment?” respondents placed a high importance on improved quality of life:
Guideline-based first-line treatment of metastatic disease for patients with intermediate/poor risk has several options. Based on the NCCN guidelines, category 1 options include axitinib + pembrolizumab, cabozantinib + nivolumab, ipilimumab + nivolumab, and lenvatinib + pembrolizumab. Similarly, the EAU guidelines state we should “offer either nivolumab + ipilimumab, pembrolizumab + axitinib, lenvatinib + pembrolizumab, or nivolumab + cabozantinib to treatment-naïve patients with IMDC intermediate or poor risk disease” (Strength rating: Strong). Despite these excellent combination therapies, there are non-responders to our current first-line treatment regimens for intermediate/poor risk metastatic clear cell RCC, given that the objective response rates to treatment range from ~30-60%:
Thus, Dr. Psutka notes that it is fair to say that most patients with clear cell RCC either do not respond to front line therapy or develop resistance to treatment. This is further emphasized when we look at progressive disease rates, which range from ~5-11%. Targeting all known actionable mechanisms in clear cell RCC with a triple combination of IO/IO + TKI therapy seems to be a logical approach in order to increase efficacy and decrease initial resistance.
In 2020, Apolo and colleagues assessed the safety and efficacy of cabozantinib + nivolumab and cabozantinib + nivolumab + ipilimumab in patients with metastatic urothelial carcinoma and other genitourinary malignancies.1 Among 54 patients (3 with RCC), treatment included eight dose levels, leading to Grade 3/4 treatment-related adverse events in 75% and 87% of patients receiving cabozantinib + nivolumab and cabozantinib + nivolumab + ipilimumab, respectively. Based on this study, the recommended phase 2 dose was cabozantinib 40 mg/day + nivolumab 3 mg/kg for the doublet therapy and cabozantinib 40 mg/day, nivolumab 3 mg/kg, and ipilimumab 1 mg/kg for the triplet therapy.
Next, Apolo et al. reported results for nivolumab + ipilimumab + cabozantinib triplet combination from a discontinued arm of the phase III CheckMate 9ER trial. Among 50 patients receiving the triplet therapy, after a median follow-up of 39.1 months (range 33.4-44.5), the median progression free survival was 9.9 (95% CI 5.7-16.8) months by BICR and 13.9 (95% CI 7.3-24.7) months by investigator. The median overall survival was 37.0 (95% CI 31.8-not estimable) months, and the objective response rate was 44.0% (95% CI 30.0-58.7; complete response, 8.0%) by BICR and 48.0% (95% CI 33.7-62.6; all partial responses) by the investigator. Grade 3-4 treatment-related adverse events occurred in 84.0%, most commonly alanine aminotransferase increased (20.0%), aspartate aminotransferase increased (16.0%), and hepatotoxicity (16.0%). Thus, there was rationale for the phase 3 COSMIC-313 trial.
COSMIC-313 was a phase 3 trial of cabozantinib in combination with ipilimumab + nivolumab versus ipilimumab + nivolumab.3 Patients with advanced clear-cell renal-cell carcinoma who had not previously received treatment and had intermediate or poor prognostic risk were enrolled into COSMIC-313. Patients were randomly assigned to receive cabozantinib daily in addition to nivolumab and ipilimumab or matched placebo in addition to nivolumab and ipilimumab. Patients then received nivolumab maintenance therapy (480 mg once every 4 weeks) for up to 2 years. The trial design for COSMIC-313 is as follows: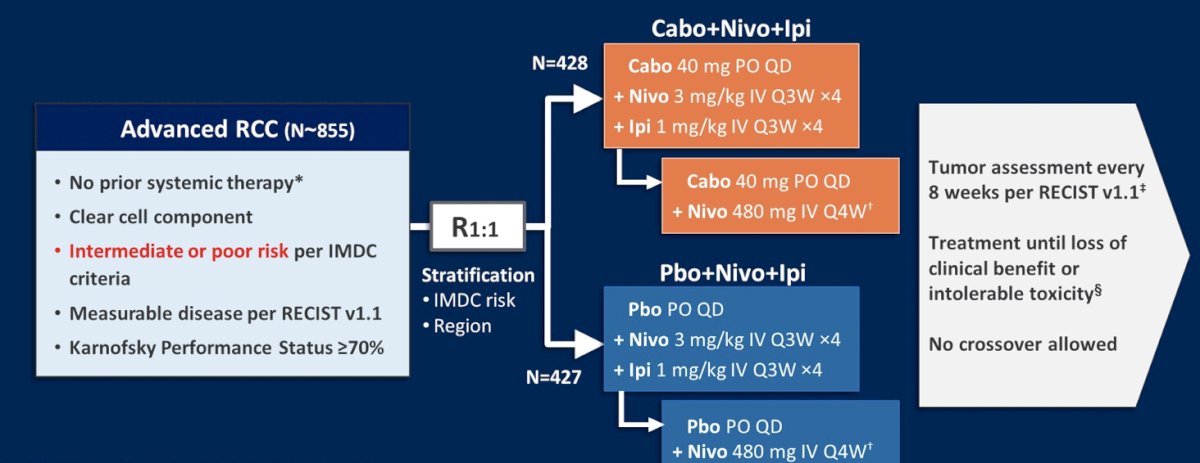
The primary end point was progression-free survival, as determined by a blinded independent review according to RECIST, v1.1. The secondary endpoint was overall survival, assessed in all patients who had undergone randomization. Among the first 550 patients that were randomized, the probability of progression-free survival at 12 months was 0.57 in the ipilimumab + nivolumab + cabozantinib group and 0.49 in the ipilimumab + group (HR 0.73, 95% CI 0.57 to 0.94):
In addition to a progression free survival benefit, there was:
- Improvement in objective response rate: 43% vs 36%
- Decreased progressive disease rate: 8% vs 20%
- Comparable complete response rate: 3% vs 3%
In this trial, 75% of patients were IMDC intermediate risk and 25% were poor risk. In patients with intermediate-risk disease in the ITT population, there was a 37% reduction in the risk of progression or death (HR 0.63, 95% CI 0.47-0.85), a benefit that was not seen in poor risk patients (HR 1.04, 95% CI 0.65-1.69):
Ultimately, the triplet therapy combination was associated with more harm compared to the doublet control arm. There were more Grade 3/4 treatment related adverse events (79% vs 56%), despite fewer patients receiving all four doses of ipilimumab (58% vs 73%), and more patients discontinuing all study treatment (12% vs 5%):
Dr. Psutka concluded COSMIC-313 noting that:
- Triplet therapy met its primary endpoint of increased median progression free survival
- However, the complete response rates were identical: 3% (low compared to pivotal ICI-ICI clinical trials)
- The overall survival signal is unknown
- There was a significant difference in Grade 3/4 adverse events
- Although inter-trial comparisons are fraught, COSMIC-313 included only intermediate and poor risk patients, with only 64% having undergone a prior cytoreductive nephrectomy, compared to other trials where 70-80% have undergone a cytoreductive nephrectomy
Thus, Dr. Psutka emphasized that triplet therapy did not meet our objective of eradicating disease and providing a cure. Moreover, it did not meet our objective of improving the other outcomes our patients care about, namely quality of life. Generally, the concerns with triplet therapy are (i) increased toxicity leading to inadequate drug delivery leading to decreased efficacy, (ii) treatment burden, (iii) qualify of life results, and (iv) financial toxicity. Additionally, there are many unknowns, particularly surrounding how frontline triplet therapy impacts future response to therapy:
- Does it change efficacy?
- Durability of response?
- Does toxicity preclude patients who progress from being able to receive future therapy?
- When we give three agents and we have a toxicity, how do we know which was the offending agent?
- What about patient selection? (benefit, ability to tolerate)
Dr. Psutka concluded her presentation discussing that for first line metastatic kidney cancer less is more emphasizing that there are a few too many unknowns:
- Triplet therapy has initial activity in intermediate and poor risk metastatic RCC with a progression free survival benefit
- There are trade-offs: Toxicity leads to treatment burden and the need for early discontinuation
- There is an unknown impact on the future, namely eligibility for further treatment and future efficacy
Presented by: Sarah Psutka, MD, MSc, Associate Professor, University of Washington, Seattle, WA
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, WellStar MCG Health, @zklaassen_md on Twitter during the 2024 European Association of Urology (EAU) annual congress, Paris, France, April 5th - April 8th, 2024
References:
- Apolo AB, Nadal R, Girardi DM, et al. Phase I Study of Cabozantinib and Nivolumab Alone or with Ipilimumab for Advanced or Metastatic Urothelial Carcinoma and Other Genitourinary Tumors. J Clin Oncol. 2020 Nov 1;38(31):3672-3684.
- Apolo AB, Powlees T, Escudier B, et al. Nivolumab plus ipilimumab plus cabozantinib triplet combination for patients with previously untreated advanced renal cell carcinoma: Results from a discontinued arm of the phase III CheckMate 9ER trial. Eur J Cancer. 2022 Dec;177:63-71.
- Choueiri TK, Powles T, Albiges, et al. Cabozantinib plus Nivolumab and Ipilimumab in Renal Cell Carcinoma. N Engl J Med. 2023 May 11;388(19):1767-1778.