(UroToday.com) The 2024 European Association of Urology (EAU) annual meeting featured a plenary session on personalized approaches in high-risk and metastatic prostate cancer, and a presentation by Dr. Alexandre De La Taille discussing that when a PSMA PET is negative for high risk disease, we cannot skip the extended pelvic lymph node dissection.
For context, this discussion was regarding a case presentation of a 51 year old with a screening PSA of 17 ng/mL, cT2 disease, with an mpMRI showing a PI-RADS 5 lesion. After a prostate biopsy, he was diagnosed with cribriform and acinar adenocarcinoma Gleason 4+4 in 5/15 cores and subsequently had negative conventional imaging and PSMA PET/CT. For his organ-confined high-risk prostate cancer, his risk of lymph node involvement (updated Briganti nomogram) was 3.2%. He underwent radical prostatectomy with extended pelvic lymph node dissection, with final pathology revealing Gleason 4+4, pT3a, pN0 (0 of 20 nodes). This patient ultimately had a lymphocele that required intervention, had a PSA persistence (0.34 ng/mL), and subsequently received salvage radiotherapy + 2 years of ADT.
Dr. De La Taille notes that the goal of his discussion advocating for extended pelvic lymph node dissection in this patient is to prove that (i) we have guidelines, (ii) extended pelvic lymph node dissection can improve survival, (iii) we cannot trust a negative PSMA PET and ‘old’ nomograms, and (iv) that negative PSMA PET patients have better outcomes. Dr. De La Taille highlighted the importance of going back to the basic science of the guidelines for high risk prostate cancer patients, reviewing statements for high-risk localized disease/locally advanced disease, and statements for extended pelvic lymph node dissection:
Dr. De La Taille notes that based on historical literature, extended pelvic lymph node dissection provides accurate staging but also reduces the risk of prostate cancer specific mortality by 23% in lymph node positive patients.1,2 Thus, if radical prostatectomy is performed in intermediate and high-risk prostate cancer, an extended pelvic lymph node dissection should be the option of choice. Moreover, at this point in time, Dr. De La Taille argues that based on a prospective multi-center trial and the OSPREY trial,3 we cannot trust a negative PSMA PET based on sensitivities for detection of ~40%. Additionally, Dr. De La Taille cautions that nomograms have too much variability, highlighting that the updated Briganti nomogram suggests this patient has only a 3.2% risk of lymph node involvement, whereas the Amsterdam-Brisbane-Sydney nomogram suggests the risk is 35.2%: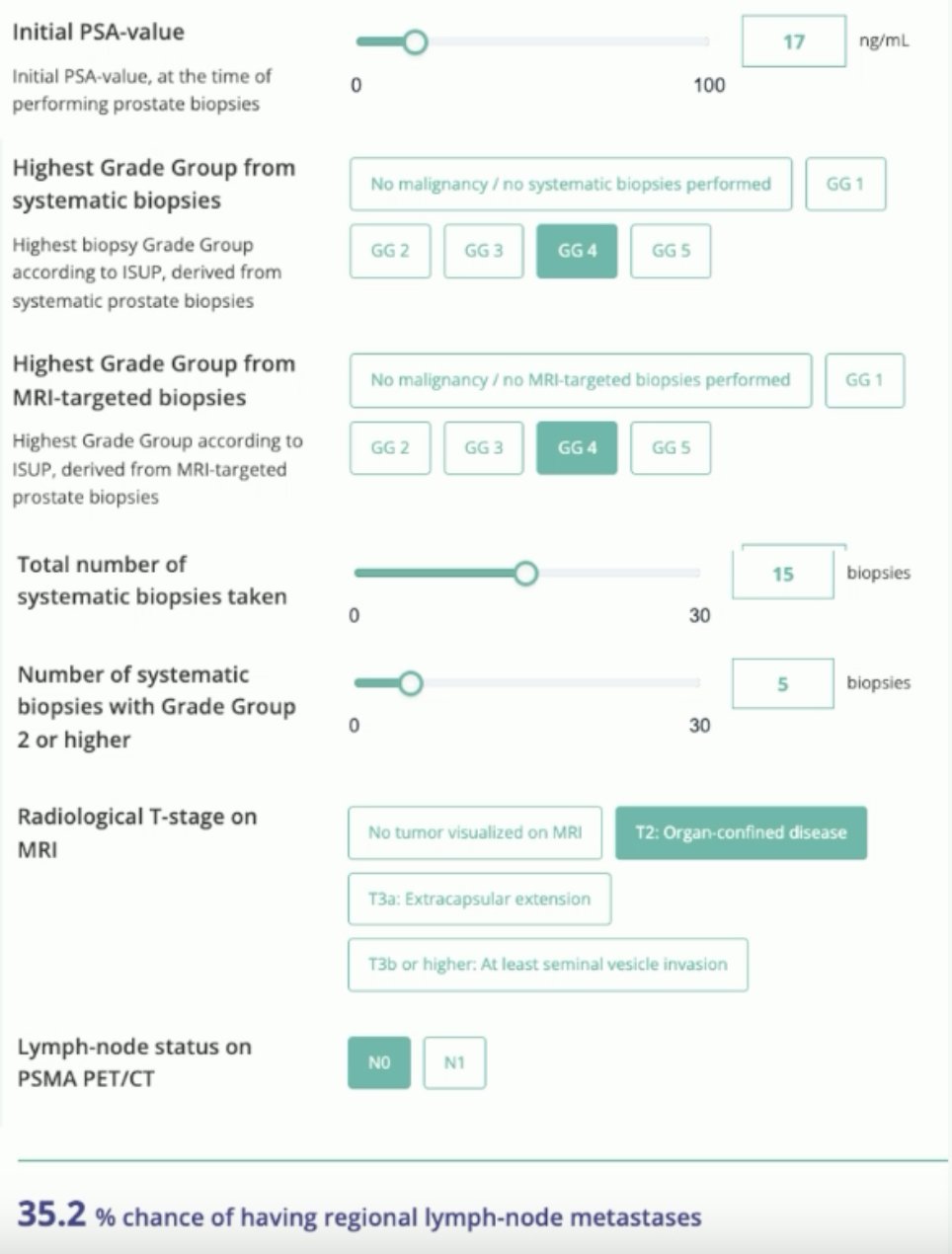
Finally, Dr. De La Taille made the argument that patients with a negative preoperative PSMA PET have better outcomes. A recent study from Marra et al. assessed 1163 pN+ men out of whom 95 and 100 had preoperative PSMA and/or Choline PET/CT, respectively.4 Of note, patients with cN+ on PSMA PET/CT had an increased risk of systemic progression (52.9% vs. 13.6% cN0 PSMA PET/CT vs. 21.5% cN0 at conventional imaging; p < 0.01). Thus, PSMA PET/CT cN+ patients with negative conventional imaging have an increased risk of systemic progression after radical prostatectomy compared to patients with cN0M0 disease both at conventional and/or molecular imaging.
Dr. De La Taille concluded his presentation discussing that when a PSMA PET is negative for high risk disease, we cannot skip the extended pelvic lymph node dissection with the following conclusions:
- No, we cannot trust a negative PSMA PET/CT
- We must be careful with the interpretation of nomograms
- We should be doing an extended pelvic lymph node dissection for (i) the best evaluation of disease extension, (ii) adapting adjuvant treatment strategies, and (iii) perhaps improving survival for these patients
Presented by: Professor Alexandre De La Taille, PUPH, MD, PhD, Hopitaux Universitaires Henri Mondor, University of Creteil, Créteil, France
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, WellStar MCG Health, @zklaassen_md on Twitter during the 2024 European Association of Urology (EAU) annual congress, Paris, France, April 5th - April 8th, 2024
References:
- Bader P, Burkhard FC, Markwalder R, et al. Is a limited node dissection an adequate staging procedure for prostate cancer. J Urol. 2002 Aug;168(2):514-518.
- Heidenreich A, Ohlmann CH, Polyakov S. Anatomical extent of pelvic lymphadenectomy in patients undergoing radical prostatectomy. Eur Urol. 2007 Jul;52(1):29-37.
- Pienta KJ, Gorin MA, Rowe SP, et al. A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J Urol. 2021 Jul;206(1):52-61.
- Marra G, Rajwa P, Filippini C, et al. The prognostic role of preoperative PSMA PET/CT in cN0M0 pN+ prostate cancer: A multicenter study. Clin Genitourin Cancer. 2024 Apr;22(2):244-251.