(UroToday.com) The 2024 European Association of Urology (EAU) annual meeting featured an upper tract urothelial carcinoma session and a presentation by Dr. Giuseppe Basile discussing a head-to-head comparison of the American Urological Association (AUA) and EAU risk stratification models of upper tract urothelial carcinoma. The EAU and the AUA have developed separate risk stratification models to guide the treatment selection process of patients with upper tract urothelial carcinoma. The AUA risk model identifies favorable and unfavorable characteristics but does not consider dimension as a major feature. The EAU risk model identifies high-risk patients if any of the features are present. As such, at the EAU 2024 annual meeting, Dr. Basile presented the results of a head-to-head comparison between the EAU and AUA risk models in predicting oncological outcomes after conservative treatment of upper tract urothelial carcinoma.
This study relied on a prospectively maintained database of patients who underwent conservative treatment for upper tract urothelial carcinoma at a tertiary care institution between 2015-2022. Patients were categorized into low-risk and high-risk subgroups according to AUA and EAU models. Second, Kaplan-Meier curves estimated the 2-year upper tract urothelial carcinoma recurrence-free survival and clinical progression defined as upgrading, upstaging or metastatic progression in low-risk and high-risk patients according to AUA and EAU models. Differences between curves were evaluated with the log-rank test. The discriminative ability of the models in predicting oncological outcomes was assessed using Harrell’s c-index. Decision-curve analysis was used to evaluate the net benefit of the predictive models.
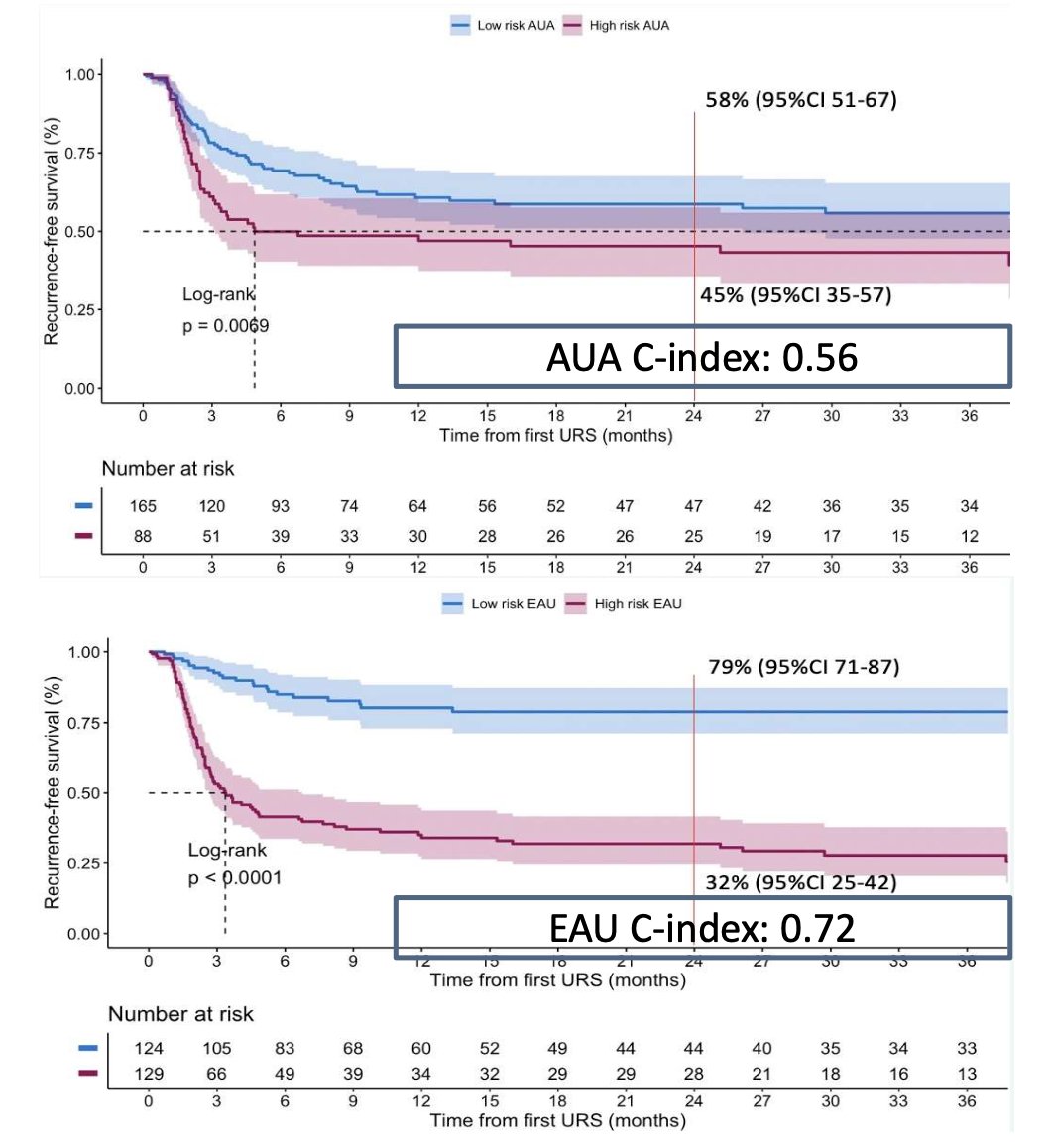
There were 165 (65%) and 88 (35%) patients categorized as low-risk and high-risk by the AUA model, respectively. Conversely, 124 (49%) and 129 (51%) were low-risk and high-risk according to the EAU model, respectively. The median follow-up was 27 (IQR: 10-42) months. Overall, 33% vs 15% low-risk patients and 50% vs 63% high-risk patients underwent radical nephroureterectomy in the AUA and EAU groups, respectively. The estimated 2-year recurrence-free survival rates were 58% (95% CI 51-67) vs 45% (95% CI 35-57) in low-risk vs high-risk (p= 0.007) for the AUA model (c-index: 0.56), and 79% (95% CI 71-87) vs 32% (95% CI 25-42) in low-risk vs high-risk (p < 0.001) for the EAU model (c-index: 0.72):
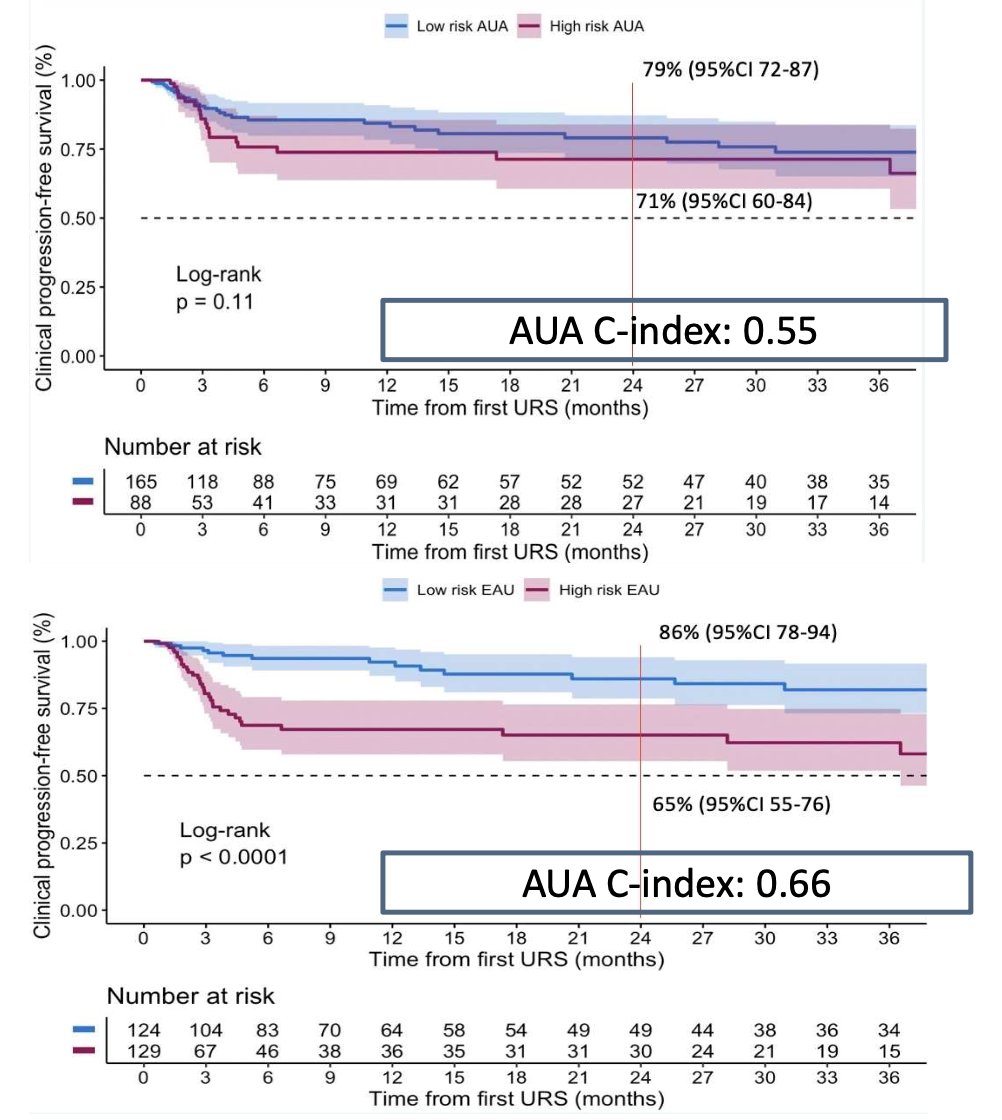
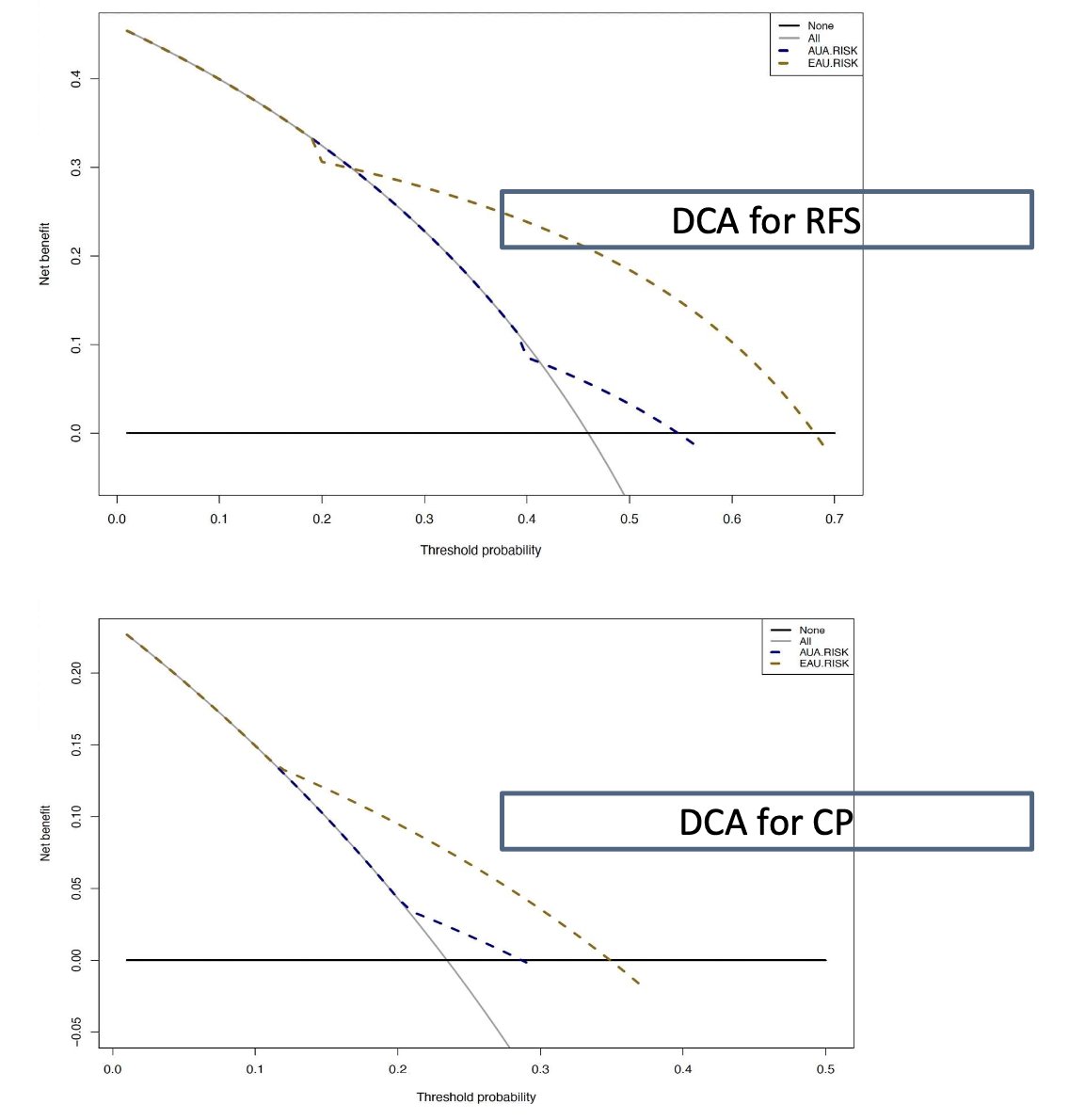
Net benefits were achieved for threshold probabilities higher than 20% and 40% for the EAU and AUA models, respectively. The estimated 2-year clinical progression rates were 79% (95% CI 72-87) vs 71% (95% CI 60-84) in low-risk vs high-risk (p = 0.10) for the AUA model (c-index: 0.55), and 86% (95% CI 78-94) vs 65% (95% CI 55-76) in low-risk vs high-risk (p < 0.001) for the EAU model (c-index: 0.66):
The decision curve analysis showed a superior net benefit for the EAU model compared to the AUA model in predicting upper tract urothelial carcinoma recurrence and clinical progression between risk classes:
Dr. Basile concluded his presentation by discussing a head-to-head comparison of the AUA and EAU risk stratification models of upper tract urothelial carcinoma with the following conclusions:
- Although both the AUA and EAU risk stratification models are useful in stratifying patients with high or low risk of disease recurrence and progression after conservative treatment, a non-negligible difference in terms of performance accuracy exists among the models
- The EAU risk stratification model showed better discriminative value in predicting clinical events compared to the AUA model
- However, considering the outcomes of contemporary series of upper tract urothelial carcinoma treated with conservative treatment, a novel risk model sharing features of the AUA and EAU models, should be developed
Presented by: Giuseppe Basile, MD, Fundació Puigvert, Dept. of Urology, Barcelona, Spain
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 European Association of Urology (EAU) annual congress, Paris, France, April 5th – April 8th, 2024