This can be done in three settings during AS:
- mpMRI at the time of initial diagnosis.
- mpMRI before a confirmatory biopsy.
- mpMRI during follow-up.
One of the ultimate goals of active surveillance is the possibility to spare follow-up biopsies in the setting of a mpMRI non-suspicious for clinically significant prostate cancer. At the Active Surveillance vs Focal Therapy in Prostate Cancer presentation at EAU 2019, Dr. Stefano Luzzago and colleagues presented results of their experience using mpMRI among men on active surveillance and the possibility of reducing the number of biopsies. Their aim was to evaluate the pathological outcomes of men enrolled in an active surveillance program and submitted to repeated mpMRIs during that time.
This study assessed 455 patients from 2006 to 2018 who were enrolled in active surveillance. All patients met PRIAS criteria and were scheduled to 1, 3 and 7-year surveillance-biopsies, and repeated 1.5-T mpMRIs. If a suspicious lesion (i.e. PI-RADS ≥3) was seen at repeated mpMRI, 2-3 cores from the target area were taken using a cognitive targeted approach. Radiological upgrading was defined as switching from a lower to a higher PI-RADS score at repeated mpMRIs. Imaging upstaging was calculated as a significant increase in the maximum diameter of the lesion (i.e. ≥2 mm). Pathological progression was defined as Gleason score upgrading at repeated biopsies and/or at the time of radical prostatectomy. Sensitivity, specificity, PPV and NPV were evaluated for radiological upgrading, imaging upstaging, both of them (upgrading + upstaging) and overall radiological progression (upgrading or upstaging).
Among these 455 men, 177 (40%) had two mpMRIs, 71 (16%) had 3, 23 (5%) had 4 and 5 (1%) men had 5 repeated mpMRIs. Median time on active surveillance was 36 (21-60) months. There were 89 (50%) men that underwent 3 prostate biopsies and 32 (18%) patients that underwent 4. The findings of the baseline (first) mpMRI are as follows:
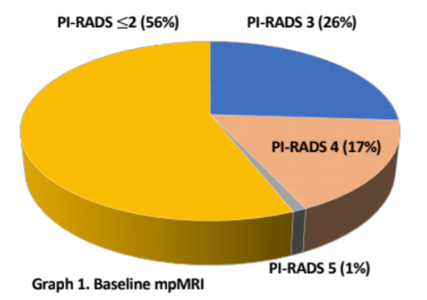
During active surveillance, the modality of radiographic progression was as follows:
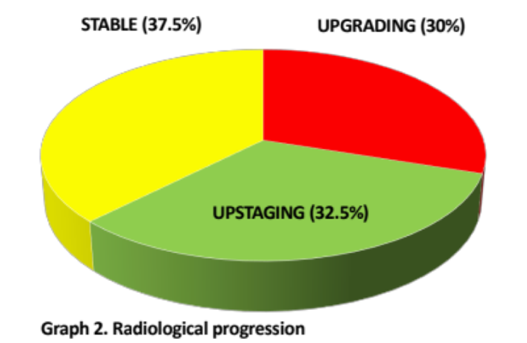
After a median follow-up of 29 (13.25-50) months, 34 (20%) men were switched to active treatment. Moreover, 21 (62%) patients showed a pathological upgrading. Of the latter, 14 (66.6%), 12 (57%), 11 (52.5%) and 15 (71%) developed radiological upgrading, upstaging, both of them and overall imaging progression, respectively. Radiological upgrading showed a PPV of 26% and a NPV of 94%. The PPV of imaging upstaging was 21% and the NPV was 92.5%. Moreover, the combination of both upgrading + upstaging showed a PPV of 31.5% and a NPV of 93%. Finally, PPV of overall radiological progression was 20% and the NPV was 94%.
With the increasing prevalence of mpMRIs, particularly in the active surveillance setting, studies such as this one from Italy are important for gathering data regarding who may be able to safely avoid follow-up biopsies based on their mpMRI findings.
The authors concluded that during active surveillance, the possibility to spare repeated biopsies in patients without radiological progression should be taken into account since only 6-8% of them harbor clinically significant prostate cancer. However, patients showing radiological progression should not be directly switched to active treatment because of the relatively low PPV of repeated mpMRIs – these patients should still have a targeted biopsy.
Presented by: Stefano Luzzago, European Institute of Oncology, Department of. Urology, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University - Medical College of Georgia, Twitter: @zklaassen_md at the 34th European Association of Urology (EAU 2019) #EAU19 conference in Barcelona, Spain, March 15-19, 2019.
References:
1. Briganti A, Fossati N, Catto JWF, et al. Active surveillance for low-risk prostate cancer: The European Association of Urology Position in 2018. Eur Urol 2018 Sep;74(3):357-368.