As mentioned above, the authors utilized the Institute of clinical evaluative sciences (ICES) data – which is a broad repository of clinical data of all patients treated in Ontario, with high level of granularity recorded. This was a retrospective population-based study using data from the Institute of clinical evaluative sciences (ICES), including all male patients aged 65 and above in Ontario who have had a negative first prostate biopsy between 1994 and 2016. In this population, they assessed the impact of commonly prescribed medications on risk of having an additional biopsy, risk of PC diagnosis and risk of PCa death. The analyzed medications included Statins (hydrophilic and hydrophobic), most commonly used diabetes drugs (metformin, insulins, sulfonylureas, and thiazolidinediones), PPIs, 5 alpha reductase inhibitors, and alpha blockers. Importantly, medication exposure was time-varying – it was modeled as “ever” vs. “never” use or as cumulative exposure.
A total of 51,415 men were analyzed over a mean (SD) follow-up time of 8.06 (5.44) years. Overall, 10,466 patients (20.4%) were diagnosed with PC, 16,726 (32.5%) had died, and 1,460 (2.8%) patients died of PC. Ultimately, following exclusions, 21,562 men were analyzed (49%) – and of these, 24% were diagnosed with PCa and 3% died of PCa.
The table below highlights the different medication classes utilized in this reduced cohort:

Ultimately, for all 3 outcomes, regardless of looking at medication use as bimodal (ever or never) or cumulative use (over 3 months), hydrophilic statins were the only predictor of receiving another biopsy, being diagnosed with PCa or dying of PCa – even when accounting for all other medication classes, age, PSA. The MV analysis for PCa diagnosis is below:
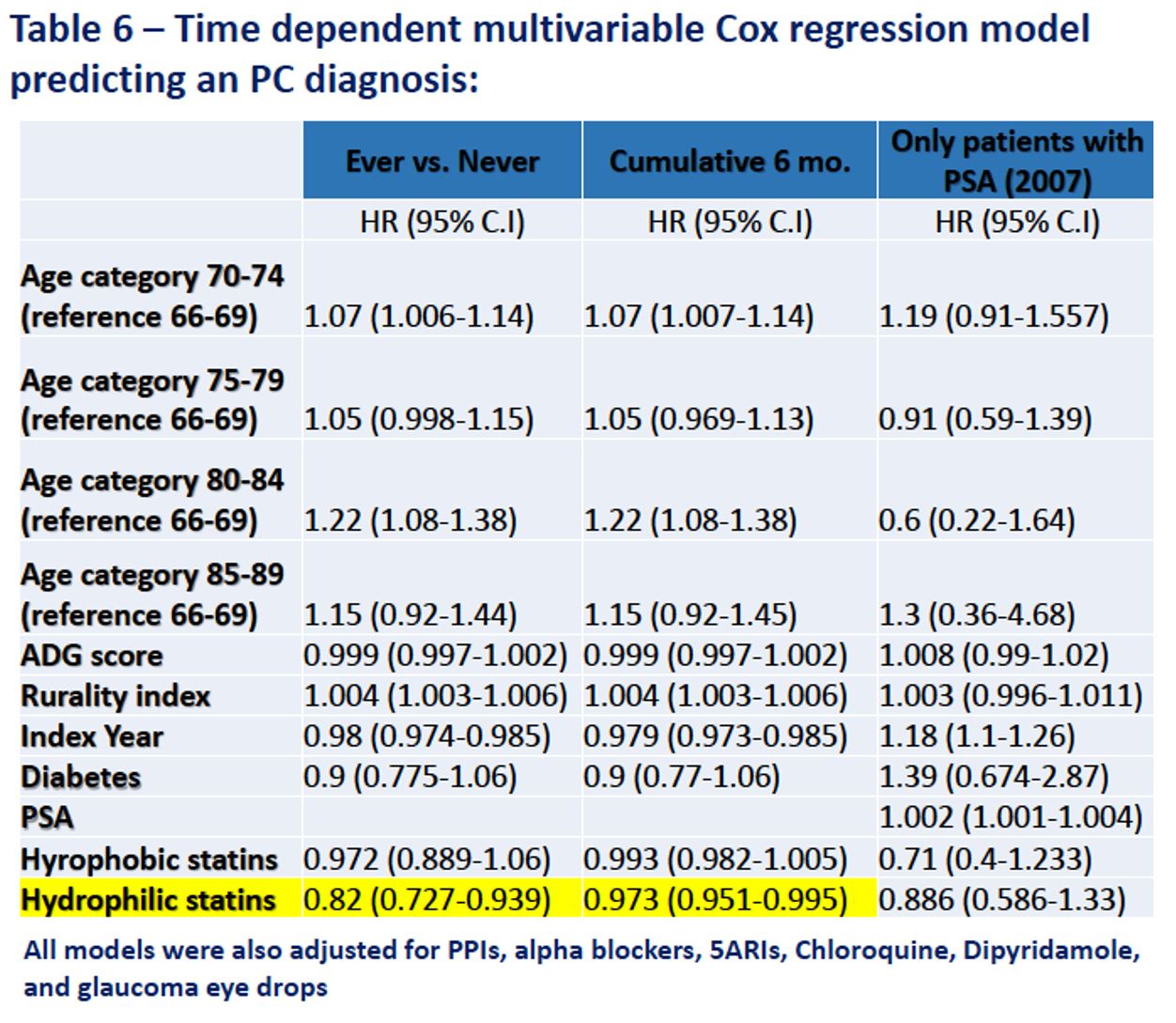
On multivariable analysis for PC diagnosis increasing age and rurality index were associated with higher PC diagnosis rate, while a more recent index year was associated with a lower diagnosis rate in both “ever” vs. “never” and cumulative models.
The MV model for PCa deaths is below:

For PCa death, hydrophobic statins were also associated with reduced mortality – albeit attenuated compared to hydrophilic statins.
The authors note that the separation of statins into hydrophobic and hydrophilic statins is a novel finding. While there have previously been studies demonstrating the potential benefits of statins as a class in PCa diagnosis, recurrence, and deaths, the effect has been weak. However, by separating into distinct categories, as only this type of dataset can, they identify a specific association with hydrophilic statins and reduced prostate cancer biopsies, PCa diagnosis and PCa deaths.
This is a very intriguing study that potentially identifies a class of agents that may have a previously unknown significant impact of PCa prevention – further work into the mechanism of action and utility in a prospective study is required.
Presented by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Toronto, Canada
Written by: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University, twitter: @tchandra_uromd, @TjuUrology at the 34th European Association of Urology (EAU 2019) #EAU19, conference in Barcelona, Spain from March 15-19, 2019.
On multivariable analysis for PC diagnosis increasing age and rurality index were associated with higher PC diagnosis rate, while a more recent index year was associated with a lower diagnosis rate in both “ever” vs. “never” and cumulative models.
The MV model for PCa deaths is below:
For PCa death, hydrophobic statins were also associated with reduced mortality – albeit attenuated compared to hydrophilic statins.
The authors note that the separation of statins into hydrophobic and hydrophilic statins is a novel finding. While there have previously been studies demonstrating the potential benefits of statins as a class in PCa diagnosis, recurrence, and deaths, the effect has been weak. However, by separating into distinct categories, as only this type of dataset can, they identify a specific association with hydrophilic statins and reduced prostate cancer biopsies, PCa diagnosis and PCa deaths.
This is a very intriguing study that potentially identifies a class of agents that may have a previously unknown significant impact of PCa prevention – further work into the mechanism of action and utility in a prospective study is required.
Presented by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Toronto, Canada
Written by: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University, twitter: @tchandra_uromd, @TjuUrology at the 34th European Association of Urology (EAU 2019) #EAU19, conference in Barcelona, Spain from March 15-19, 2019.