However, more recently, a subset of patients with oligometastatic disease are increasingly being recognized – and even men with clinically node-positive disease (with very low volume metastatic disease elsewhere) are being offered cytoreductive prostatectomy as part of the clinical trial. We know from the Messing data and others that a subset of men with pN1 disease following RP does well without any systemic therapy. Yet, how do we best select the men that are likely to benefit from localized therapy in the presence of cN+ disease?
In this study, 274 men with imaging detected cN1 PCa treated with RP and lymph node dissection (LND) between 2005 and 2018 at three international tertiary referral centers were identified. Clinical Recurrence (CR) was defined as the onset of metastases detected by imaging during follow-up. CSM = cancer-specific mortality, or prostate cancer-specific mortality. They then completed a regression tree analysis and stratified patients into risk groups based on clinical and preoperative characteristics; this was to identify patients at risk for CR and those not at risk.
Full Demographics of the group is shown below:

The median number of clinically suspicious nodes was 1. 84% had GG 3-5 on pre-RP biopsy. Node-positive disease was noted on either conventional (CT/MRI; n=227; 82.8%) or more recent functional approaches (PSMA/Choline PET/CT; n=47; 17.2%). The median number of nodes removed was 18, with 3 nodes being positive. Of the entire population, 80% and 20% of patients had pelvic vs. retroperitoneal ± pelvic lymphadenopathies; the second group had a more advanced cN+ disease. The median size of positive nodes at imaging was 13 mm. 148 (55%) men received neoadjuvant androgen deprivation therapy (ADT) – which is not currently recommended. 209 (77%) patients had pathological lymph node invasion – meaning 23% were pN0 despite being cN+. Median follow-up was 64 months or approximately 5 years.
Following RP, 179 (66%) and 52 (19%) patients received ADT and aRT. The use of ADT was based on the evidence from the Messing data.
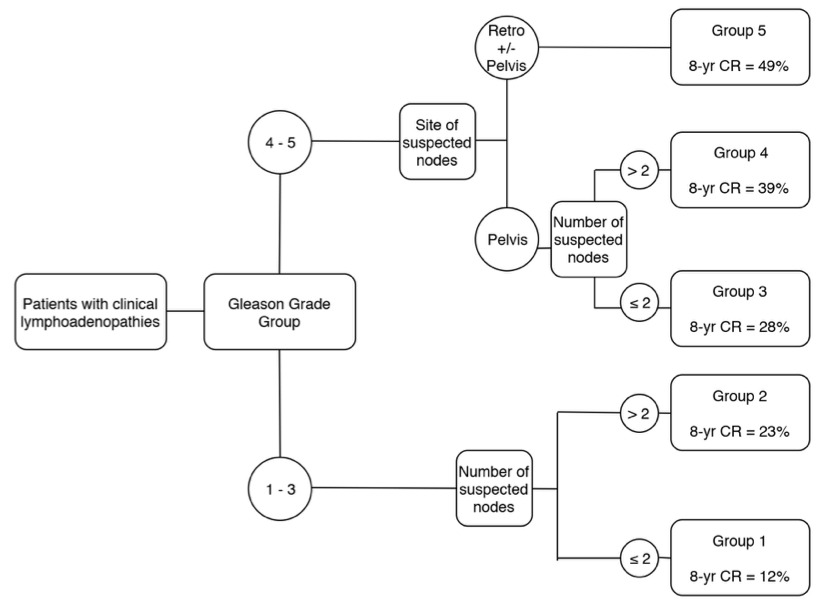
On regression analysis, biopsy GG, site of nodal disease, and the number of suspicious nodes on pre-operative imaging were the primary predictors of CR. The full model is seen below:

1. Very low risk: grade group 1–3 and ≤2 lymphadenopathies: 8-year CR: 12%
2. Low risk: biopsy grade group 1–3 and >2 lymphadenopathies; 8-year CR: 23%
3. Intermediate risk: grade group 4–5 and ≤2 pelvic lymphadenopathies; 8-year CR: 28%;
4. High risk: grade group 4–5 and >2 pelvic lymphadenopathies; 8-year CR: 39%;
5. Very high risk: grade group 4–5 and retroperitoneal lymphadenopathies; 8-year CR: 49%.
The c-index of this tool was 72% in terms of discriminating CR outcomes. It’s not a perfect tool but may help guide patient selection. The authors note that surgery (or local therapy) might play a role in selected patients with biopsy grade group 1-3 and/or enlarged nodes only in the pelvis in the setting of a multi-modal approach. A grade group 4-5 disease and lymphadenopathies in the retroperitoneum are associated with worse oncological outcomes and these patients should be considered for systemic therapies upfront thus sparing the morbidity associated with local treatment.
Presented by: Giorgio Gandaglia, MD, Division of Oncology/Unit of Urology, URI, IRCCS Ospedale San Raffaele, Milan, Italy
Written by: Thenappan Chandrasekar, MD (Clinical Instructor, Thomas Jefferson University) (twitter: @tchandra_uromd, @TjuUrology) at the 34th European Association of Urology (EAU 2019) #EAU19, conference in Barcelona, Spain, March 15-19, 2019.
References:
1. Messing EM, Manola J, Sarosdy M, Wilding G, Crawford ED, Trump D. Immediate hormonal therapy compared with observation after radical prostatectomy and pelvic lymphadenectomy in men with node-positive prostate cancer. N Engl J Med. 1999 Dec 9;341(24):1781-8.