(UroToday.com) The 2022 EAU annual meeting featured a session on improvements in metastatic prostate cancer focusing on imaging and treatment, including a presentation by Dr. Nicolaas Lumen discussing the changing landscape of systemic therapy in the treatment of newly-diagnosed metastatic prostate cancer. Phase 3 trials have proven the benefit of adding 2nd line systemic treatment to ADT in newly-diagnosed metastatic prostate cancer. These 2nd line treatments include docetaxel, abiraterone acetate and apalutamide and are guideline-recommended to be combined with ADT in newly-diagnosed metastatic prostate cancer. At the 2022 EAU meeting, Dr. Lumen and colleagues describe the changes in systemic treatment of newly-diagnosed metastatic prostate cancer in a “real-world” setting. In addition, they explored the reasons of non-compliance to adding 2nd line systemic treatment to the patient’s regimen.
Since 2014, patients with newly-diagnosed metastatic prostate cancer were prospectively registered. For this study, patients were divided into 4 time periods:
- Group 1: January 2014-July 2015
- Group 2 after introduction of docetaxel: August 2015-July 2017
- Group 3 after introduction of abiraterone acetate: August 2017-February 2018
- Group 4 after introduction of apalutamide: March 2018-October 2021

For every time period, Dr. Lumen evaluated the initiated systemic treatment. In case the patient received a treatment that was not compliant with strong recommendations in the contemporary guidelines, the reason for non-compliance was further extrapolated.
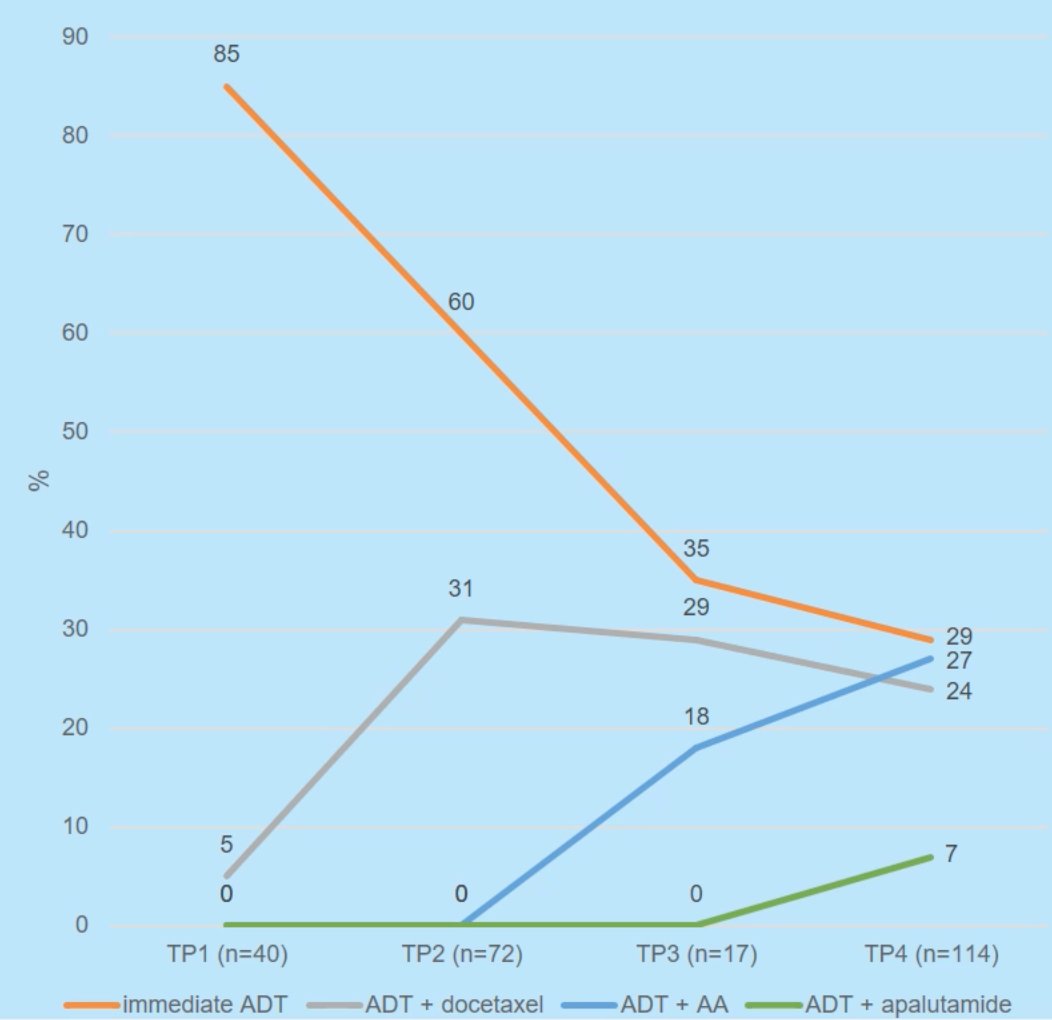
In total, 243 patients were included. There were significant changes in the type of systemic treatment that was initiated across the 4 time periods, including a gradual decrease in treatment with only ADT, ADT + docetaxel use ranging from 24-31% utilization, and abiraterone and apalutamide use increasing over time:
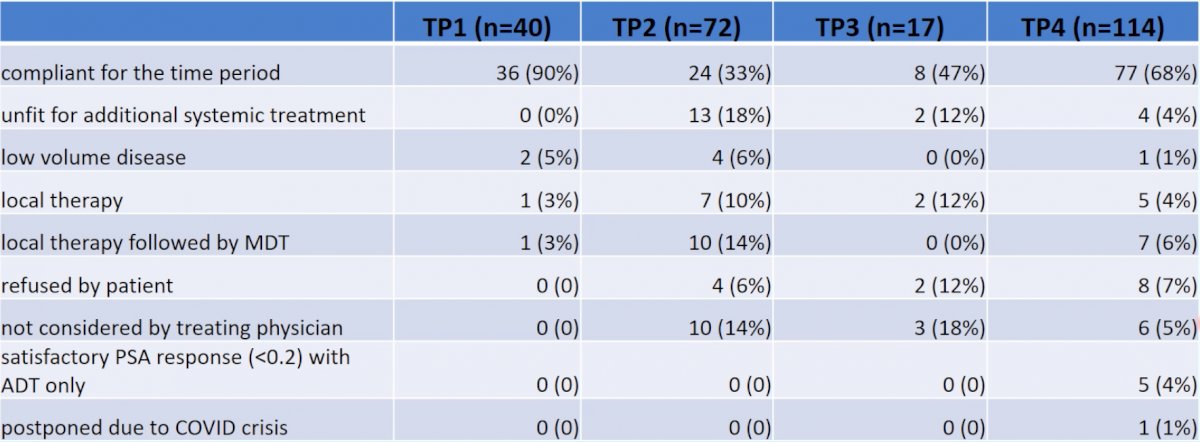
Sixty percent of patients were treated in accordance to the contemporary guidelines. The reasons for non-compliance were heterogeneous and varied across the 4 time periods, but generally included decreased treatment for patients that were unfit for treatment intensification in Groups 3 and 4:
Dr. Lumen concluded this presentation discussing the changing landscape of systemic therapy in the treatment of newly-diagnosed metastatic prostate cancer with the following take home messages:
- The use of ADT only (early or deferred) declined gradually after the introduction of 2nd line treatments
- The proportion of patients unfit to undergo 2nd line systemic treatment declined after abiraterone acetate and apalutamide became available
Presented by: Nicolaas Lumen, MD, PhD, Ghent University Hospital, Dept. of Urology, Ghent, Belgium
Co-Authors: Lambert E.1, Fonteyne V.2, De Maeseneer D.3, Van Praet C.1
Affiliations: 1Ghent University Hospital, Dept. of Urology, Ghent, Belgium, 2Ghent University Hospital, Dept. of Radiation Oncology, Ghent, Belgium, 3Ghent University Hospital, Dept. of Medical Oncology, Ghent, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 European Association of Urology (EAU) Annual Hybrid Meeting, Amsterdam, NL, Fri, July 1 – Mon, July 4, 2022.