(UroToday.com) The 2022 EAU annual meeting featured a session on improvements in metastatic prostate cancer focusing on imaging and treatment, including a presentation by Dr. Simona Malaspina discussing the implications of PSMA-flare after ADT evaluated with 18F-PSMA-1007 PET/CT in hormone-sensitive metastatic prostate cancer. Short-term ADT increases heterogeneously PSMA-uptake (PSMA-flare) in PET imaging of hormone-sensitive prostate cancer. Dr. Malaspina and colleagues hypothesized that lesions having PSMA-flare might have a different potential to respond to ADT or progress. This prospective trial aimed to investigate the PSMA-flare phenomenon and to observe whether FDG PET might provide additional molecular imaging information, given that aggressive prostate cancer tends to display glucose uptake.
This prospective, registered (NCT03876912) trial enrolls patients with newly diagnosed metastatic (M1) prostate cancer. All patients undergo 18F-PSMA-1007 PET/CT before and 3-4 weeks after the initiation of Degarelix (240 mg). At baseline 18F-FDG PET/CT is also performed:
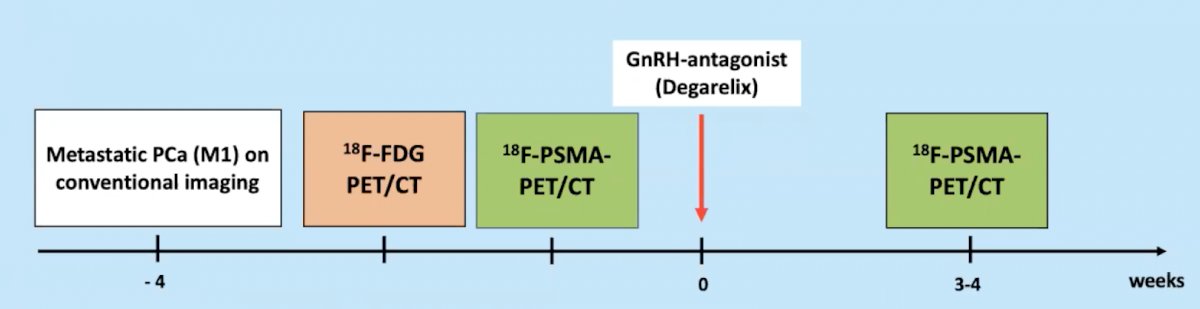
Standardized uptake value (SUV)max on primary tumour and metastatic lesions is calculated in all PET scans. The increase, decrease or no-change of PSMA-uptake after ADT is represented as ΔSUVmax.
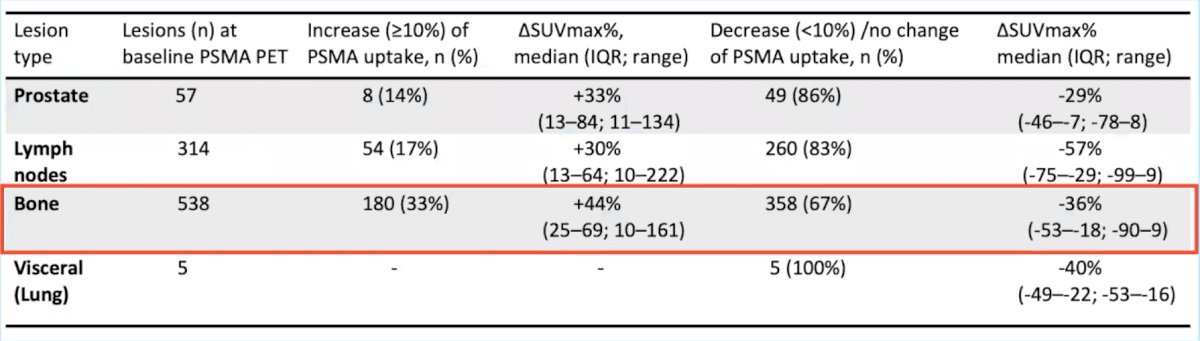
To date, 25 patients (mean age: 71 years; median PSA: 45 ng/ml, range 15-3400) completed all scans. All patients reached castration levels (testosterone < 1.7 nmol/L) at the time of the second PSMA PET/CT, performed within a median of 25-days (range 17-33) after initiation of ADT. All patients had bone and nodal disease, 5 patients had also visceral metastases. In total 538 bone, 314 lymph nodes, 57 prostate, and 5 visceral lesions were analyzed. After ADT, 180 (33%) bone, 54 (17%) lymph nodes, and 8 (14%) prostate lesions showed an increase (>10%) of PSMA uptake, with a median ΔSUVmax% of +44% (range 10-161), +30% (range 10-222) and +33% (range 13-134), respectively:
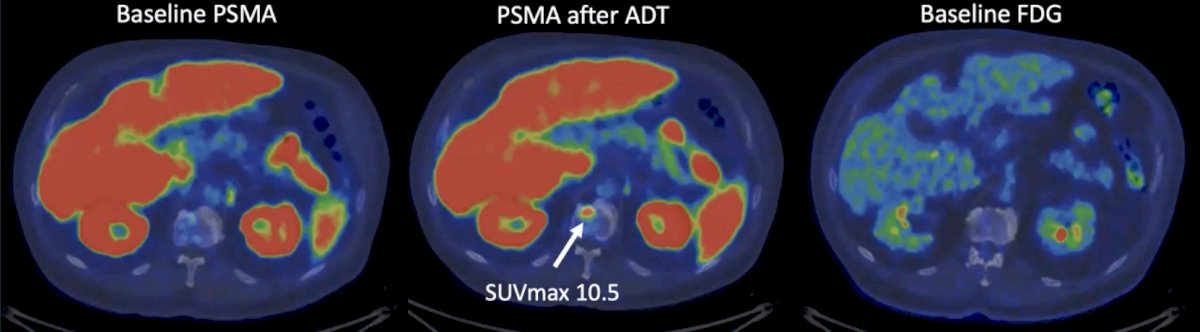
Moreover, 10 patients with known bone lesions presented with new PSMA bone uptake at the second PSMA scan:
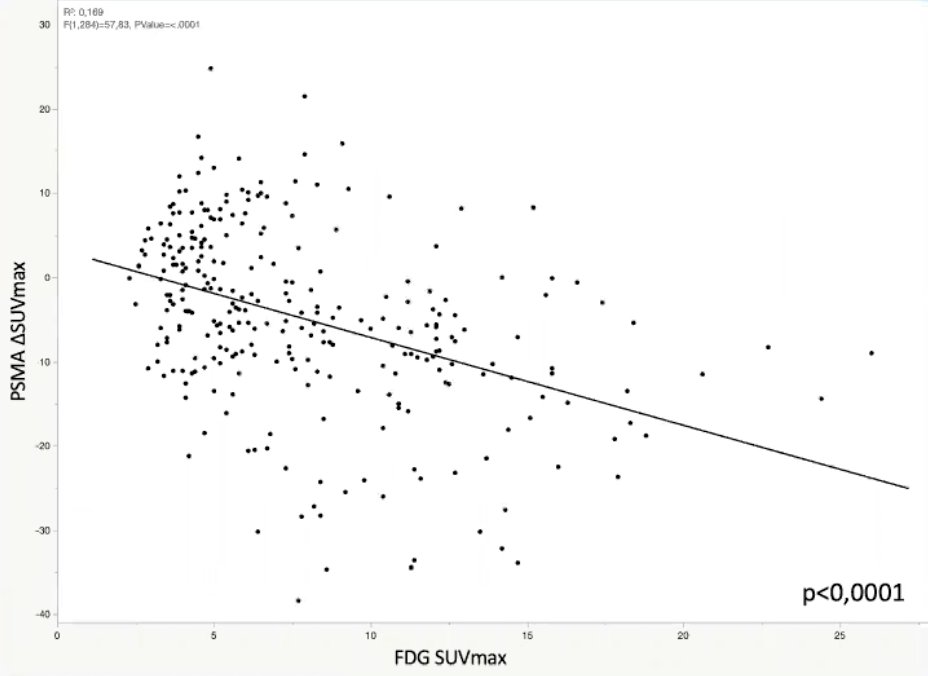
Among the bone metastases, 53% of those presenting with the PSMA-flare and 51% of those showing decrease/no change of PSMA-uptake were FDG-positive. In these lesions, the authors observed an inverse correlation (p < 0.0001) between the PSMA ΔSUVmax and FDG SUVmax intensity:
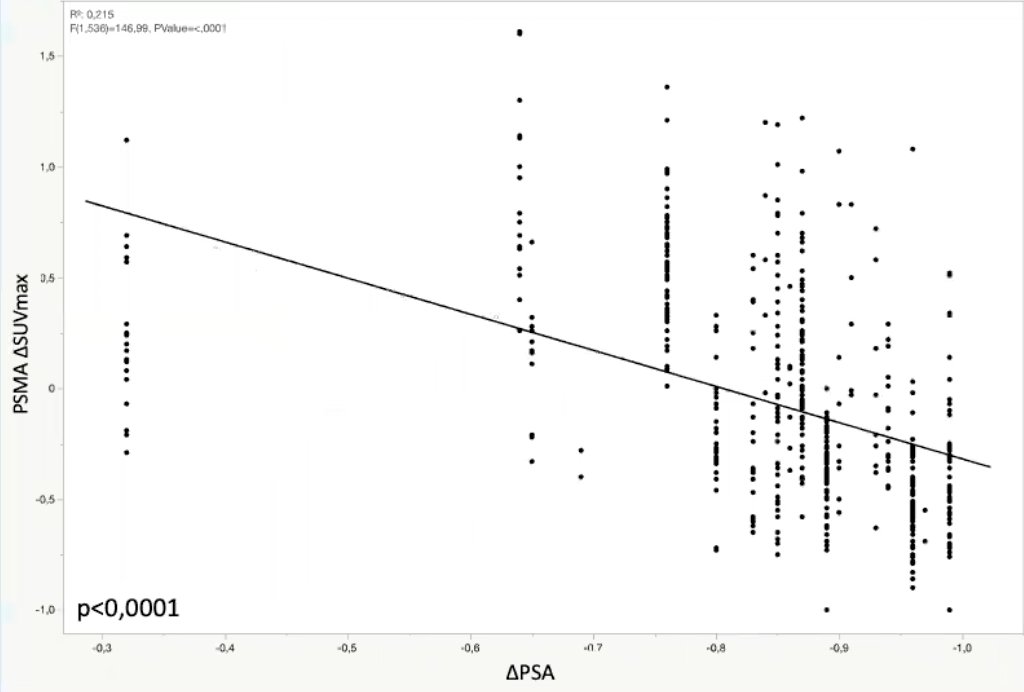
The PSMA uptake versus serum PSA in bone lesions is as follows:
Dr. Malaspina concluded her presentation discussing the implications of PSMA-flare after ADT evaluated with 18F-PSMA-1007 PET/CT in hormone-sensitive metastatic prostate cancer with the following take-home messages:
- A heterogeneous increase in PSMA uptake after short-term ADT was detected in treatment-naïve metastatic prostate cancer patients, most evident in the bone lesions
- A negative correlation between the PSMA flare and the intensity of glucose uptake, as well as the decrease of serum PSA was observed
- Lesions presenting with PSMA flare might potentially be less aggressive and have better response to ADT
Presented by: Simona Malaspina, MD, Turku University Hospital and University of Turku, Turku PET Centre, Turku, Finland
Co-Authors: Ettala O.2, Tolvanen T.1, Forsback S.1, Boström P.J.2, Kemppainen J.1
Affiliations: 1Turku University Hospital and University of Turku, Turku PET Centre, Turku, Finland, 2Turku University Hospital and University of Turku, Dept. of Urology, Turku, Finland
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 European Association of Urology (EAU) Annual Hybrid Meeting, Amsterdam, NL, Fri, July 1 – Mon, July 4, 2022.