Dr. Rocco began his discussion by mentioning the history of NS. Up to 1982, virtually all men who underwent surgical treatment for prostate cancer were impotent after surgery. Pieter J. Donker and Patrick C. Walsh discovered the cavernous nerves during a dissection performed in a stillborn male infant on February 13, 1981. In 1982 the first purposeful NS RP was performed. One year following the procedure, the patient reported normal sexual function, and 25 years later the patient was with an undetectable PSA and stable quality of life.
Dr. Rocco moved on to discuss the fascias of the prostate. The pelvic fascias are either parietal or visceral. The parietal component covers the medial aspects of the levator ani muscles. The visceral component of the endopelvic fascia covers the pelvic organs. These include the prostate, bladder, and rectum, and it is fused with the anterior fibromuscular stroma of the prostate at the upper ventral aspect of the gland. Along the pelvic sidewall, the parietal and visceral components of the endopelvic fascia are fused. This fusion is recognizable as a whitish line named fascial tendinous arch of the pelvis (Figure 1).
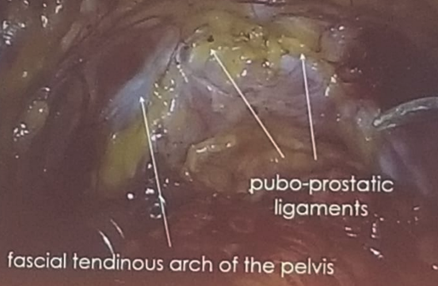
Figure 1 – The fascial tendinous arch of the pelvis
The periprostatic fascia is the fascia on the outer surface of the prostate. The lateral thickened fascial band components of the dorsal vein complex (DVC) are called Walsh’s pillars.
The neurovascular bundle was next discussed by Dr. Rocco. The inferior hypogastric plexus or pelvic plexus is responsible for the mechanism of erection, ejaculation, and urinary continence. The dense neural network of the pelvic plexus lies within a fibrofatty, flat, rectangular, sagittaly oriented plate between the bladder and the rectum (Figure 2).

Figure 2 – The neural network of the pelvic plexus between the bladder and rectum:
Finally, Dr. Rocco elaborated on the performance of NS. The concept of NS has gone through several changes over the years. In the beginning, there was the concept of all or none NS, which later evolved to traditional complete NS, partial NS or non-NS. Recently, a grading system has been formulated to include five different grades of NS (Figure 3):
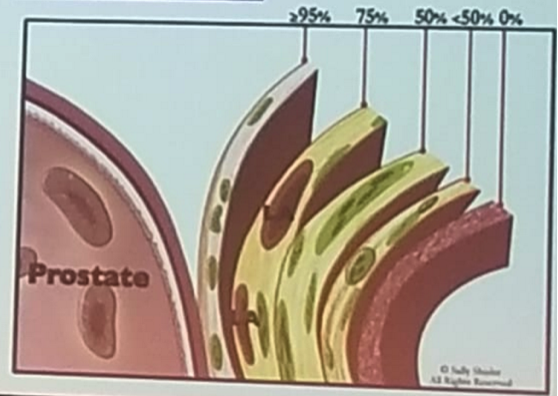
Figure 3 – Grades of nerve-sparing:
1= No NS
2 = <50% NS
3 = 50% NS
4 = 75% NS
5 = 95% NS
There is an online nomogram helping to predict the amount of extracapsular extension, thus informing us what kind of NS should be attempted, if any (www.prece.it).
Presented by: B. Rocco, Modena, Italy
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter:@GoldbergHanan at the EAU Robotic Urology Section (ERUS) Meeting - September 5 - 7, 2018 - Marseille, France