Dr. Panebianco notes that the diagnostic work-up for hematuria typically includes abdomino-pelvic imaging and cystoscopy as first line tests, with diagnostic transurethral resection of bladder tumors (TURBT) for confirmatory pathology. Total body CT scan or FDG-PET/CT is typically reserved for muscle-invasive bladder cancer (MIBC) staging, whereas a bladder MRI is used for local staging. She notes that TURBT has a diagnostic inaccuracy of 23-50%, including 7-30% of non-muscle-invasive bladder cancer (NMIBC) being understaged, including up to 45% of patients when detrusor muscle is absent.
The rationale and aim of VI-RADS were to define a standardized approach to imaging and reporting mpMRI for bladder cancer, defining the risk of muscle invasion.1 Furthermore, VI-RADS was created through a consensus using existing literature. The scoring is applicable to untreated patients and to treated patients having only received a diagnostic TURBT, but prior to re-TURBT. mpMRI is best performed before or at least 2 weeks after TURBT, bladder biopsy, or intravesical treatment. Administration of an intramuscular antispasmodic agent is recommended, in addition to adequate bladder distention. MRI does not necessarily have the ability to visualize all of the histological bladder wall layers, however, it is able to assess size, location, multiplicity, and morphology. A 5-point VI-RADS score is generated using the individual T2W, DWI, and DCE MRI categories and suggests the probability of muscle invasion. The dominant sequences for risk estimates are DWI (first) and DCE (second, especially if DWI is sub-optimal). The T2 sequence (structural category) is helpful as a first pass guide.
The VI-RADS 1.0 scoring is as follows:
- VI-RADS 1: SC CE and DW category 1 (muscle invasion is highly unlikely)
- VI-RADS 2: SC, CE, and DW category 2; both CE and DW category 2 with SC category 3 (muscle invasion is unlikely to be present)
- VI-RADS 3: SC, CE, and DW category 3; SC category 3, CE or DW category 3, and the remaining sequence category 2 (the presence of muscle invasion is equivocal)
- VI-RADS 4: At least SC and/or DW and CE category 4; the remaining category 3 or 4 SC category 3 plus DW and/or CE category 4; SC category 5 plus DW and/or CE category 4 (muscle invasion is likely)
- VI-RADS 5: at least SC plus DW and/or CE category 5; the remaining category 4 or 5 (invasion of muscle and beyond the bladder is very likely)

Dr. Panebianco notes that since their initial publication in 2018, there have been several studies that have provided (retrospective) validation of the scoring system, with a high interrader-agreement:
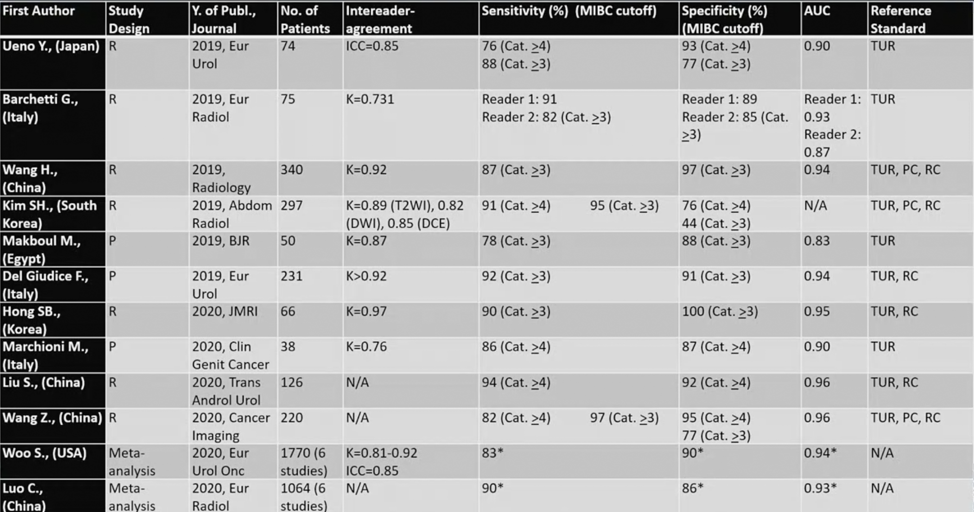
A recently published meta-analysis also provides further data with regards to VI-RADS’ diagnostic performance.2 Luo et al. assessed six studies with 1,064 patients included in the analysis. The pooled sensitivity, specificity, and AUC value were 0.90 (95% CI 0.86-0.94), 0.86 (95% CI 0.71-0.94), and 0.93 (95% CI 0.91-0.95) for VI-RADS 3 as the cutoff value. The corresponding estimates were 0.77 (95% CI 0.65-0.86), 0.97 (95% CI 0.88-0.99), and 0.92 (95% CI 0.89-0.94) for VI-RADS 4 as the cutoff value. Based on these results, the authors concluded that VI-RADS can provide a good predictive ability for detecting the muscle invasiveness of primary bladder cancer with VI-RADS 3 or VI-RADS 4 as a cutoff value.
Dr. Panebianco states that what is next after validation is to establish a new bladder cancer MRI VI-RADS pathway.3 Dr. Panebianco’s group recently published a study prospectively validating VI-RADS for discrimination between NMIBC and MIBC at TURBT, and evaluated the accuracy of VI-RADS for identifying high-risk NMIBC patients who could avoid re-TURBT and detecting those at higher risk for understaging after TURBT.4 There were 231 patients with bladder cancer suspicion that were offered mpMRI before TURBT, and according to VI-RADS, a cutoff of ≥3 to define MIBC was assumed. mpMRI showed sensitivity, specificity, PPV, and NPV for discriminating NMIBC from MIBC at initial TURBT of 91.9% (95% CI 82.2-97.3), 91.1% (95% CI 85.8-94.9), 77.5% (95% CI 65.8-86.7), and 97.1% (95% CI 93.3-99.1), respectively. Furthermore, the AUC was 0.94 (95% CI 0.91-0.97). Among HR-NMIBC patients (n=114), mpMRI before TURBT showed sensitivity, specificity, PPV, and NPV of 85% (95% CI 62.1-96.8), 93.6% (95% CI 86.6-97.6), 74.5% (95% CI 52.4-90.1), and 96.6% (95% CI 90.5-99.3) respectively, to identify patients with MIBC at re-TURBT (AUC 0.93, 95% CI 0.87-0.97).
During the COVID-19 pandemic, VI-RADS has the potential to be even more important in the management of NMIBC. Dr. Panebianco and colleagues suggest that VI-RADS may have a role in the initial diagnostic workup for gross hematuria, in the selection of patients with high-risk NMIBC for restaging transurethral resection, and assessment for neoadjuvant regimen administration for locally advanced disease.5
Dr. Panebianco concluded with several take-home messages from her presentation discussion the continued emergence of VI-RADS:
- VI-RADS can assess risk of muscle invasion
- There are several MRI pathways for increasing patient satisfaction:
- NMIBC versus MIBC (ie. no TURBT for patients with VI-RADS 1-2)
- VI-RADS 3 or VI-RADS 4 can predict muscle-invasiveness
- T2 MIBC versus locally advanced bladder cancer (T3-T4) (ie. sampling TURBT for confirmatory pathology in patients with VI-RADS 5)
- Assessing response to therapy (also in the neoadjuvant setting based on data from PURE-01)
- Surveillance of NMIBC for young patients
Presented by: Valeria Panebianco, MD, Sapienza/Policlinico Umberto, Rome, Italy
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 12th European Multidisciplinary Congress on Urological Cancers (EMUC) (#EMUC20 ), November 13th - 14th, 2020
References:
- Panebianco V, Narumi Y, Altun E, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting and Data System). Eur Urol 2018 Sep;74(3):294-306.
- Luo C, Huang B, Wu Y, et al. Use of Vesical Imaging-Reporting and Data System (VI-RADS) for detecting the muscle invasion of bladder cancer: A diagnostic meta-analysis. Eur Radiol. 2020 Aug;30(8):4606-4614.
- Panebianco V, Narumi Y, Barchetti G, et al. Should we perform multiparametric magnetic resonance imaging of the bladder before transurethral resection of bladder? Time to reconsider the rules. Eur Urol 2019 Jul;76(1):57-58.
- Del Giudice F, Barchetti G, De Berardinis E, et al. Prospective assessment of Vesical Imaging Reporting and Data System (VI-RADS) and its Clinical Impact on the Management of High-risk non-muscle-invasive bladder cancer patients candidate for repeated transurethral resection. Eur Urol 2020 Jan;77(1):101-109.
- Panebianco V, Del Giudice F, Leonardo C, et al. VI-RADS Scoring Criteria for Alternative Risk-adapted Strategies in the Management of Bladder Cancer During the COVID-19 Pandemic. Eur Urol 2020 Jul;78(1):e18-e20.