In survey data presented by Dr. van der Poel, 69% of respondents note that oligometastatic prostate cancer represents a distinct biological state in comparison to polymetastatic disease. So, whether there is a utility in detecting and treating patients with oligometastatic lymph node metastasis is intriguing. Dr. van der Poel notes that based on several studies spanning prostate, bladder, and kidney cancer, for early metastases there is no associated benefit to lymph node dissection from stopping further spread of disease.
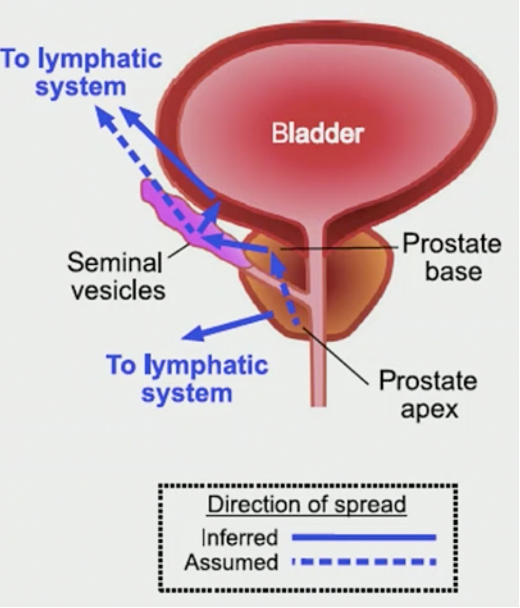
Recent work has suggested that for prostate cancer patients, routes of metastasis differ between patients, noting that local progression likely correlates with metastatic spread:
To understand the dynamics of metastasis development, Dr. van der Poel states that it is interesting to look at the Allee effect: at a low number of metastasizing cells, resources are scarce and tumor growth is low. When vascular invasion increases in the metastases, tumor cell proliferation rapidly increases until it is so overwhelming that cancer cell death occurs in the center of the tumor, sending clusters of cells from the tumor throughout the body and supporting the hypothesis that metastasis may develop from existing metastatic sites. The Allee effect suggests that in early development of low volume metastasis, surgical resection may still be effective:
An important question is whether we can ascertain an optimal window in which surgical resection or radiotherapy to a metastatic site is clinically useful. In a squamous cell carcinoma setting, a polyclonal model of metastatic dissemination has been proposed, whereby distinct clones were seen in metastatic sites showing a pattern of intimate intermixing, and as such prevention of intermixing may improve outcomes.
According to the National Institute of Health, oligometastases is defined as “a type of metastasis in which cancer cells from the original (primary) tumor travel through the body and form a small number of new tumors (metastatic tumors) in one or two other parts of the body. These types of tumors may be treatable.” However, Dr. van der Poel notes that in current metastasis directed therapy trials, there is significant heterogeneity among inclusion criteria for the number of metastases, ranging from <3-10 metastatic lesions. When dealing with patients with oligometastatic disease it is important to consider prognostic factors available when selecting those that may benefit from treatment:
- Young age: usually defined as <65 or <70 years of age
- Patient fitness: Karnofsky performance status >=70
- Slow-growing cancers: metachronous presentation of oligometastases, or longer disease-free interval between the original tumor and development of metastases
- Minimal disease burden: the presence of few metastatic sites, or single organ oligometastases, as well as a lack of extracranial disease
Dr. van der Poel concluded with the following take-home messages:
- Biology
- Metastases arise early, variably and are likely polyclonal
- Genetic and immunomodulatory aspects likely determine progression
- Oligometastases occur prior to clonal intermixing
- Definitions
- <6 locations
- 1-2 organ systems
- Longer interval to the primary tumor
Presented by: Henk G. van der Poel, MD, The Department of Urology, The Netherlands Cancer Institute, Amsterdam, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 12th European Multidisciplinary Congress on Urological Cancers (EMUC) (#EMUC20 ), November 13th - 14th, 2020