Androgen deprivation therapy (ADT) is the mainstay of the therapy of metastatic PC. However, initial treatment responses to ADT are transitory, and with time, patients will progress to metastatic castration-resistant prostate cancer (mCRPC).
Radium-223 dichloride (223Ra) is the first alpha particle emitting bone-seeking agent approved for mCRPC. It has a half-life of 11.4 days; it is considered safe and indicated for patients with mCRPC with symptomatic bone metastases.3 Biomarkers for 223Ra treatment and its correlation with AR-V7 splice variant are currently being investigated.
In the presented EXCAAPE study, the authors aimed to assess the activity and safety of 223Ra in asymptomatic mCRPC patients who have already progressed from first-line hormonal therapy. The authors also attempted to correlate the potential association of AR-V7 splice variant status with 223Ra efficacy.
The key inclusion criteria consisted of patients older than 18 years. Patients had to have histologically confirmed adenocarcinoma of the prostate without neuroendocrine differentiation or small cell features. All patients also had metastatic bone disease with no visceral metastases. Patients were all asymptomatic according to the intensity scale in the Brief Pain Inventory short form. Patients were also previously treated with abiraterone acetate or enzalutamide treatment for at least 24 weeks. Prior docetaxel therapy was only allowed in hormone-sensitive patients. All patients were continuously treated with ADT and bone-health supportive agents at standard doses ≥4 weeks prior to start.
This was a multicenter, single-arm, open-label, non-controlled phase IIa clinical trial.
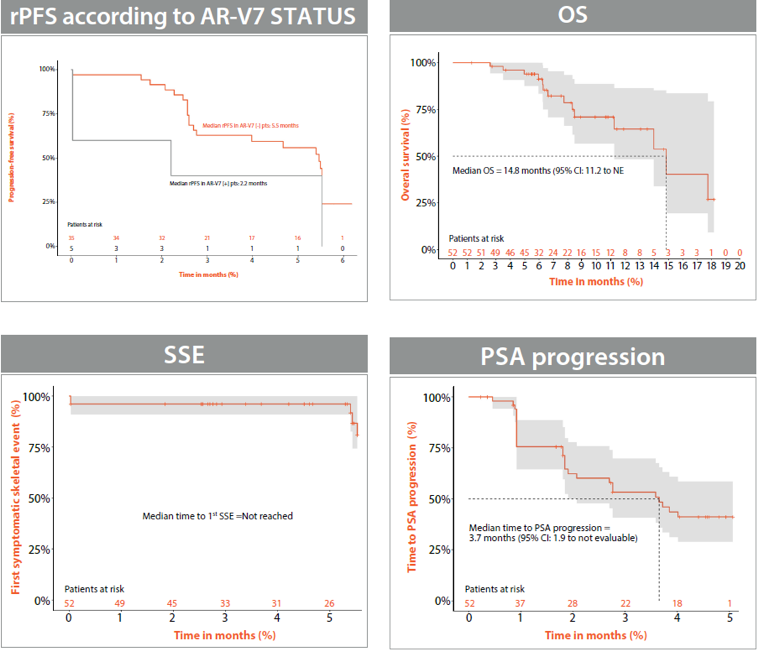
Patients were treated with IV 223Ra at a dose of 55 kBq/Kg, given at four-week intervals for six cycles. Each patient had a baseline blood sample taken to perform an analysis of circulating tumor cells (CTCs). The study's primary endpoint was radiographic progression-free survival (rPFS). Secondary endpoints included rPFS according to AR-V7 status, overall survival (OS), time to first symptomatic skeletal event (SSE), and time to prostate-specific antigen (PSA) progression.
Table 1 shows the patient characteristics of the 52 patients who were accrued for this trial from 9 centers in Spain. Figure 1 shows the results of the primary endpoint (rPFS).
Table 1 – Patient characteristics:
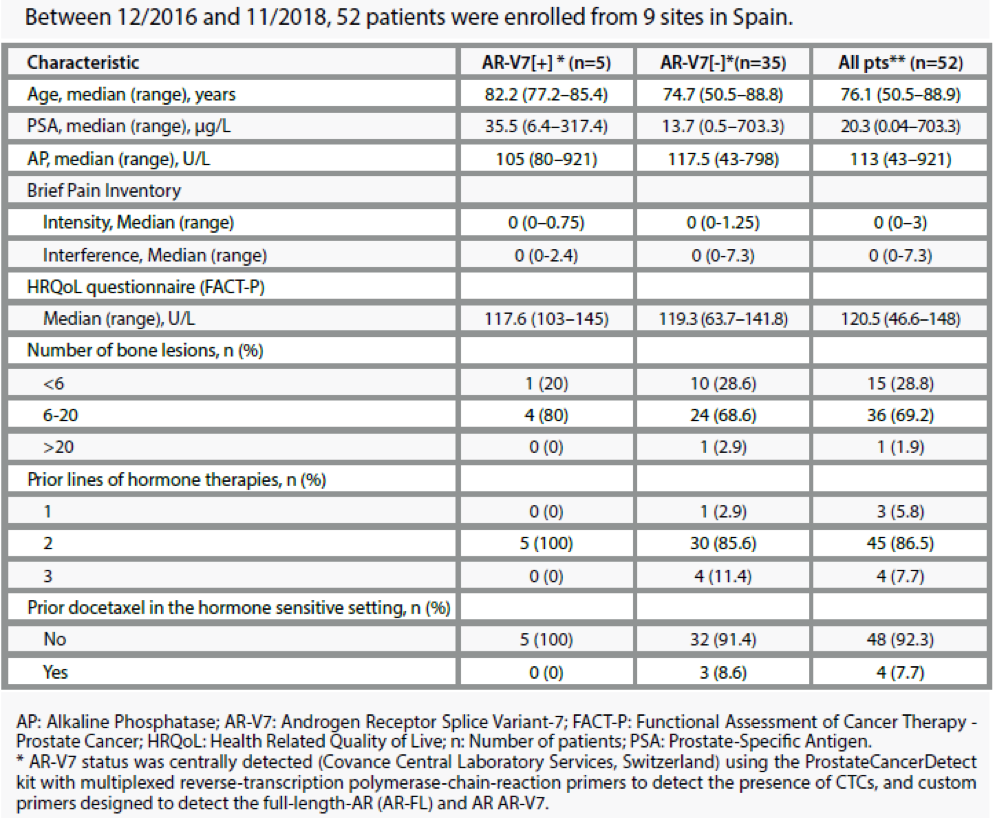
Figure 1 – rPFS of 223 Ra:
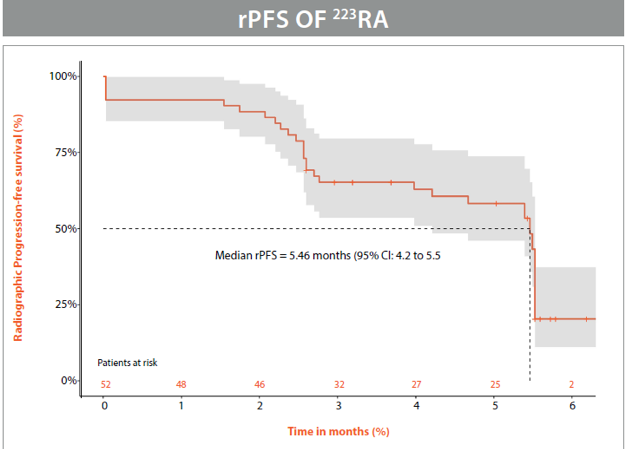
Figure 2 shows the efficacy of 223Ra with regards to ARV7 splice variant, OS, symptomatic skeletal events (SSE), and PSA progression.
Figure 2 – Efficacy of 223Ra with regards to various endpoints:
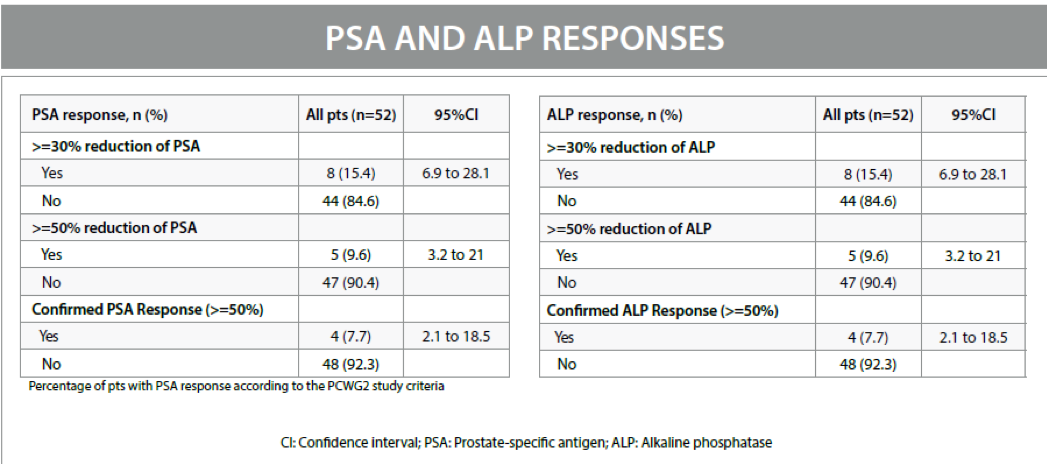
PSA and alkaline phosphatase (ALP) responses are shown in Table 2.
Table 2 - PSA and ALP responses:
When assessing the safety perspective of this treatment, all-cause adverse events (AEs) occurred in 88.5% of patients, with grade 3/4 AEs being reported in 22.1% of patients. The most frequent G3/4 AEs were anemia (11.5%) and thrombocytopenia (5.8%).
A total of 31 patients (59.6%) completed the full six cycles of treatment. 13 patients (25%) had disease progression prior to the sixth cycle, and a total of 3 patients (5.8%) withdrew their consent. Overall, five patients were discontinued from the study: 2 patients (3.8%) due to unacceptable toxicity (AE grade >3), two patients (3.8%) due to worsening of their performance status, and one patient (1.9%) due to investigator's decision. Importantly, no therapy-related deaths had occurred.
In conclusion, 223Ra was shown to be an active and safe 2nd line treatment modality in asymptomatic mCRPC bone-metastatic patients who have progressed to first-line new hormonal regimens.
Presented by: Joan Carles, MD, PhD, Oncology Department, Vall d’Hebron University Hospital, Barcelona, Spain
Written by: Hanan Goldberg, MD, MSc., Assistant Professor of Urology, SUNY Upstate Medical University, Syracuse, NY, USA, @GoldbergHanan, at the European Society for Medical Oncology Virtual Congress, ESMO Virtual Congress 2020 #ESMO20, 18 Sept - 21 Sept 2020.
References:
- Wu JN, Fish KM, Evans CP, Devere White RW, Dall'Era MA. No improvement noted in overall or cause-specific survival for men presenting with metastatic prostate cancer over a 20-year period. Cancer 2014; 120(6): 818-23.
- Berruti A, Dogliotti L, Bitossi R, et al. Incidence of skeletal complications in patients with bone metastatic prostate cancer and hormone-refractory disease: predictive role of bone resorption and formation markers evaluated at baseline. The Journal of urology 2000; 164(4): 1248-53.
- Bruland ØS, Nilsson S, Fisher DR, Larsen RH. High-Linear Energy Transfer Irradiation Targeted to Skeletal Metastases by the α-Emitter 223Ra: Adjuvant or Alternative to Conventional Modalities? Clinical Cancer Research 2006; 12(20): 6250s-7s.