(UroToday.com) The 2022 ESMO annual meeting featured a prostate cancer session, including a presentation by Dr. Evan Yu discussing the results of KEYLYNK-010, a randomized, open-label phase 3 study assessing pembrolizumab + olaparib versus abiraterone or enzalutamide for patients with previously treated mCRPC. Indeed, there is an unmet need for effective therapies for patients with heavily pretreated mCRPC. KEYLYNK-010 (NCT03834519) evaluated the efficacy and safety of pembrolizumab + olaparib vs abiraterone or enzalutamide for molecularly unselected patients with mCRPC after a next-generation hormonal agent and docetaxel.
For KEYLYNK-010, eligible patients were ≥18 years of age, had mCRPC that progressed on or after abiraterone or enzalutamide (but not both) as well as docetaxel, and had ECOG performance status ≤1. Patients were randomized 2:1 to 200 mg pembrolizumab IV Q3W for ≤35 cycles + 300 mg olaparib orally BID, or to next-generation hormonal agent: 1000 mg abiraterone orally QD (if prior enzalutamide) or 160 mg enzalutamide orally QD (if prior abiraterone):

The dual primary endpoints were radiographic PFS (rPFS) by blinded independent central review per PCWG-modified RECIST 1.1 (final testing at first interim analysis), and OS (final testing at second interim analysis). Secondary endpoints included ORR by blinded independent central review per PCWG-modified RECIST 1.1 and safety/adverse events.
There were 793 patients randomized to pembrolizumab + olaparib (n = 529) or next-generation hormonal agent (n = 264) between May 30, 2019 and July 16, 2021. Ultimately, the KEYLYNK-010 study was stopped for futility. As of January 18, 2022, the median follow-up for the second interim analysis was 11.9 months (range 0.9–31.0). Baseline characteristics were balanced between arms:

The primary endpoints of rPFS (median 4.4 months with pembrolizumab + olaparib vs 4.2 months with next-generation hormonal agent; HR 1.02, 95% CI 0.82−1.25; p = 0.55)
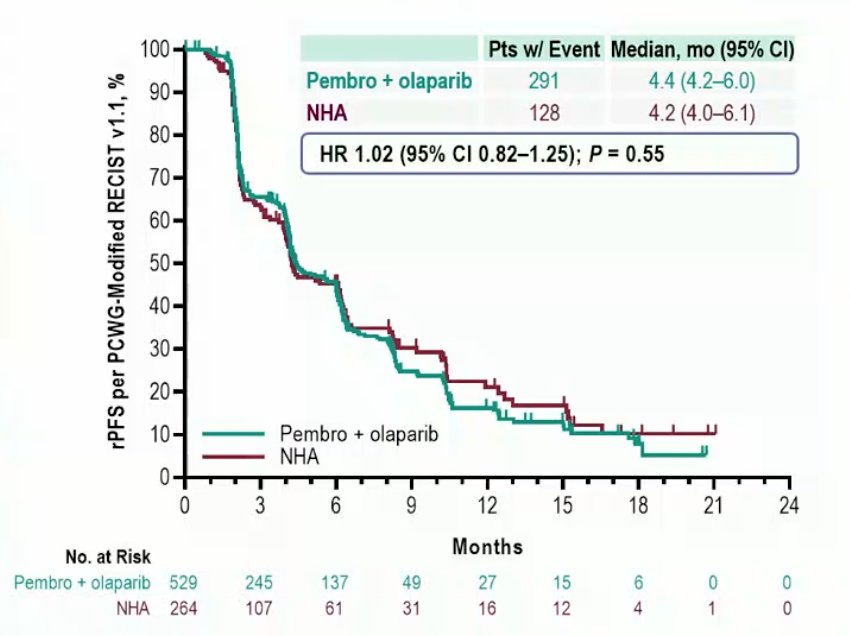
and OS (15.8 months vs 14.6 months; HR 0.94, 95% CI 0.77−1.14; p = 0.26) were not met:

Additionally, there was no difference in time from subsequent therapy between the groups (7.2 months vs 5.7 months; HR 0.86, 95% CI 0.71−1.03):

The most common subsequent therapy in both arms was cabazitaxel (pembrolizumab + olaparib 51.4% vs next-generation hormonal agent 55.3%). The ORR was 16.8% with pembrolizumab + olaparib vs 5.9% with next-generation hormonal agent (nominal p = 0.002). There were 4 (1.6%) complete responses in the pembrolizumab + olaparib and none in the next-generation hormonal agent arm. An exploratory analysis of subgroups by tissue-based homologous recombination repair gene alteration at the second interim analysis suggested a potential difference in rPFS (HRR mutations [pembrolizumab + olaparib n=81, next-generation hormonal agent n=37]: HR 0.53, 95% CI 0.33–0.86; non-HRR mutations [pembrolizumab + olaparib n=246, next-generation hormonal agent n=118]: HR 1.19, 95% CI 0.90–1.58) but not in OS (HRR mutations: HR 0.91, 95% CI 0.53–1.56; non-HRR mutations: HR 1.03, 95% CI 0.77–1.38). Grade ≥3 treatment-related adverse events occurred in 34.6% of patients with pembrolizumab + olaparib and 9.0% of patients with next-generation hormonal agent; 5% and 1% of patients, respectively, had grade ≥3 immune-mediated adverse events. The most common treatment-related adverse events (>= 5%) are as follows:

Dr. Yu concluded his presentation discussing the results of KEYLYNK-010, a randomized, open-label phase 3 study assessing pembrolizumab + olaparib versus abiraterone or enzalutamide for patients with previously treated mCRPC with the following take-home messages:
- The randomized, phase 3 KEYLYNK-010 study did not show a statistically significant improvement in rPFS or OS with pembrolizumab + olaparib versus the active comparator next-generation hormonal agent for men with molecularly unselected, previously treated mCRPC
- The study was stopped for futility after the second prespecified interim analysis based on the guidance of the external data monitoring committee
- ORR was higher in the pembrolizumab + olaparib group versus the next-generation hormonal agent group
- The safety profile of pembrolizumab + olaparib was consistent with previous reports, although there were more grade >= 3 treatment-related adverse events occurred with pembrolizumab + olaparib versus next-generation hormonal agents
- Ongoing studies are investigating other pembrolizumab- or olaparib-based combinations in prostate cancer
Presented by: Evan Yu, MD, Professor, Department of Medicine, Division of Oncology, University of Washington School of Medicine, Member, Clinical Research Division, Fred Hutchinson Cancer Research Center, Clinical Research Director, Genitourinary Oncology, Seattle Cancer Care Alliance, Medical Director, Clinical Research Service, Fred Hutchinson Cancer Research Consortium, Seattle, Washington
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 European Society of Medical Oncology (ESMO) Annual Hybrid Meeting, Paris, FR, Fri, Sept 9 – Tues, Sept 13, 2022.