(UroToday.com) The 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023 was host to a non-prostate, genitourinary tumors mini oral session. Dr. Martin H. Voss presented the results of a study evaluating MEDI5752 (volrustomig), a novel PD-1/CTLA-4 bispecific antibody, for the 1st line treatment of patients with advanced clear cell renal cell carcinoma (ccRCC).
The combination of PD-1/CTLA-4 inhibition has been shown to improve survival in the 1st line treatment for advanced clear cell RCC, especially among those with IMDC intermediate-poor risk disease. In the CheckMate-214 trial, the combination of nivolumab + ipilimumab was shown to be associated with an objective response rate of 40%, with a complete response rate of 9% and a 12-month progression-free survival rate of 12 to 40%.1
Volrustomig is a monovalent PD-1/CTLA-4 bispecific monoclonal antibody, which distinctly achieves full PD-1 blockade plus preferential CTLA-4 inhibition on activated PD-1+ T cells. At doses ≥500 mg, volrustomig enables CTLA-4 pharmacodynamic activity which is greater than that observed with clinically tolerable doses of co-formulated PDA-1 + CTLA-4. In the 1st line ccRCC setting, 1,500 mg administered every 3 weeks has promising efficacy (ORR: 58%, progressive disease <10%), but dosing is limited by immune-related adverse events (~25% with Grade 3-4 liver toxicity, AE discontinuation >70%).2 In this report, Dr. Voss presented emerging data with volrustomig 750 mg and 500 mg in the 1st line clear cell RCC setting that show encouraging activity with an improved safety profile compared to the volrustomig 1,500 mg dose.
The study design is summarized below. Patients with IO- and VEGFR-TKI-naïve ccRCC in the 1st line setting were randomized 1:1 to either volrustomig 750 mg every 3 weeks (n=32) or volrustomig 500 mg every 3 weeks (n=33). No IMDC risk restrictions were applied. The primary objective was objective response rate, with key secondary objectives of pharmacokinetics and immunogenicity.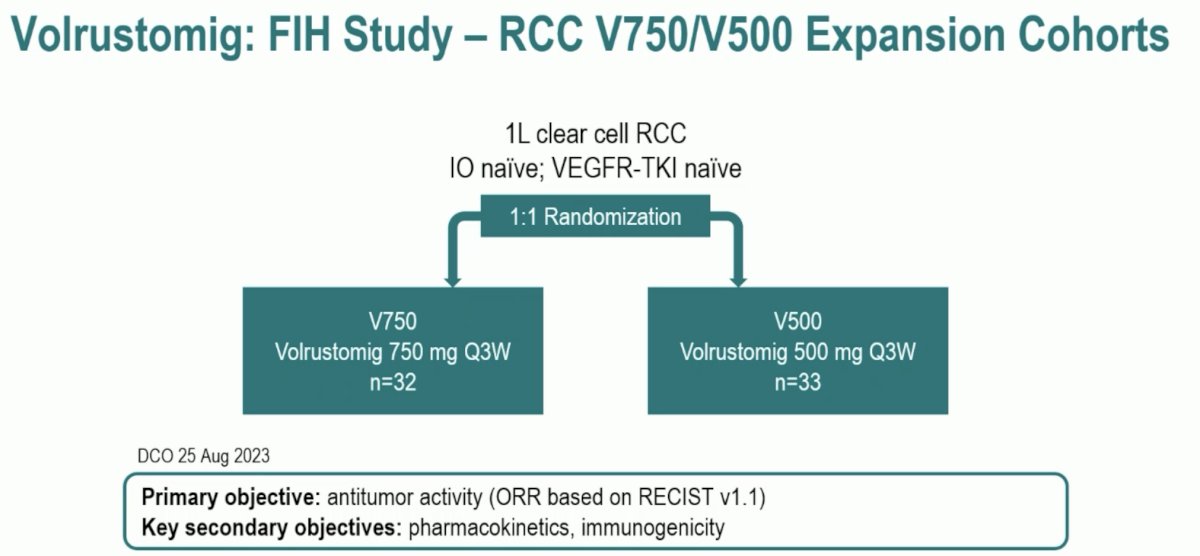
The median patient age ranged between 59 and 64 years. A prior nephrectomy was undergone in 53 – 67% of patients. 72% of patients in the 750 mg dose group had IMDC intermediate-poor risk disease, compared to 64% of those in the 500 mg dose group. High PD-L1 expression, defined as ≥1% on SP263, was present in 66% and 79% of patients in the V750 and V500 groups, respectively.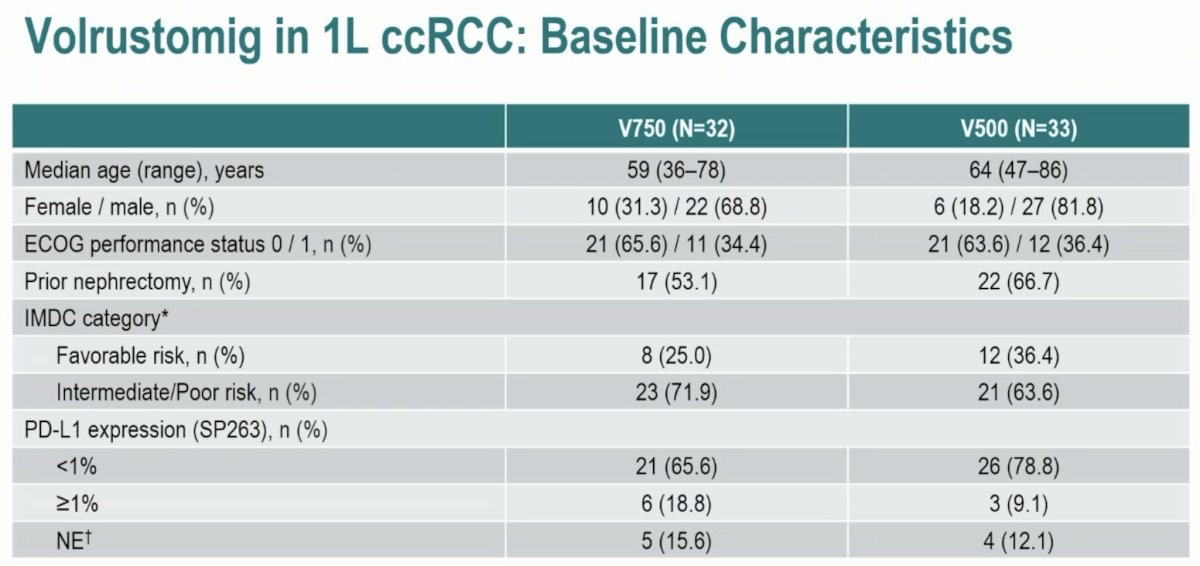
From an efficacy standpoint, the ORR was 48% with V750 and 46% with V500. The corresponding CR rates were 10% and 6%, respectively. Progressive disease was recorded in 10% and 24% of patients, respectively. The disease control rate was higher in the V750 group (90% versus 70%). The median duration of response among responders was also longer with the higher dose of 750 mg (17 versus 11.5 months).
When the ORR was stratified by IMDC risk group (favorable versus intermediate/poor), we note that among patients in the favorable risk group, the ORR was higher with the lower dose of V500 (58% versus 25%), whereas in the intermediate/poor risk group, the ORR was higher with the 750 mg dose (57% versus 38%).
The waterfall plot summarizing Volrustomig’s efficacy is demonstrated below:
The spider plots below demonstrate that the median PFS rates were 12.3 and 9.7 months in the 750 and 500 mg groups, respectively, with 12-month PFS rates of 52% and 44%, respectively
From a safety standpoint, all grade treatment-related adverse events (TRAEs) occurred in 97% and 94% of patients in the 750 and 500 mg groups, respectively. Grade 3-4 TRAEs were present in 63% and 42% of these patients, respectively. TRAE leading to treatment discontinuation occurred in 47% and 39% of patients, respectively.
As illustrated below, volrustomig at both the 750 and 500 mg doses was associated with increased T cell activation in the 1st line ccRCC setting, with pharmacodynamic effects at V750 > V500. Interestingly, volrustomig achieves T-cell proliferation and activation levels higher than those seen with doses of anti-CTLA-4 used in clinical practice.
Dr. Voss concluded as follows:
- Volrustomig monotherapy at 750 mg and 500 mg every 3 weeks is active in treatment-naive advanced ccRCC
- Responses are frequently deep and durable; V750 improves both objective response rate (especially in intermediate-poor risk groups) and primary resistance (<10%)
- Maturing data at V750 mg show promising duration of response and progression-free survival rates with a 12 month rate of 51.7%
- V750 and V500 administered every 3 weeks have an improved safety profile compared to V1500
- Volrustomig at both the 750 and 500 mg doses is associated with increased T cell activation, with pharmacodynamic effects at V750 > V500. Notably, volrustomig achieves T-cell proliferation and activation levels higher than those seen with doses of anti-CTLA-4 used in clinical practice.
- A combination of volrustomig with lenvatinib is currently being evaluated in first-line RCC (NCT04522323)
- Volrustomig has the potential to improve outcomes in patients with advanced RCC
Presented by: Martin Voss, MD, Clinical Director, Genitourinary Oncology Service at Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023
References:- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med 2018;378(14):1277-1290.
- Albiges L, Rodriguez LM, Kim S, et al. Safety and clinical activity of MEDI5752, a PD-1/CTLA-4 bispecific checkpoint inhibitor, as monotherapy in patients (pts) with advanced renal cell carcinoma (RCC): Preliminary results from an FTIH trial. J Clin Oncol. 2022;40(Suppl 16):107.